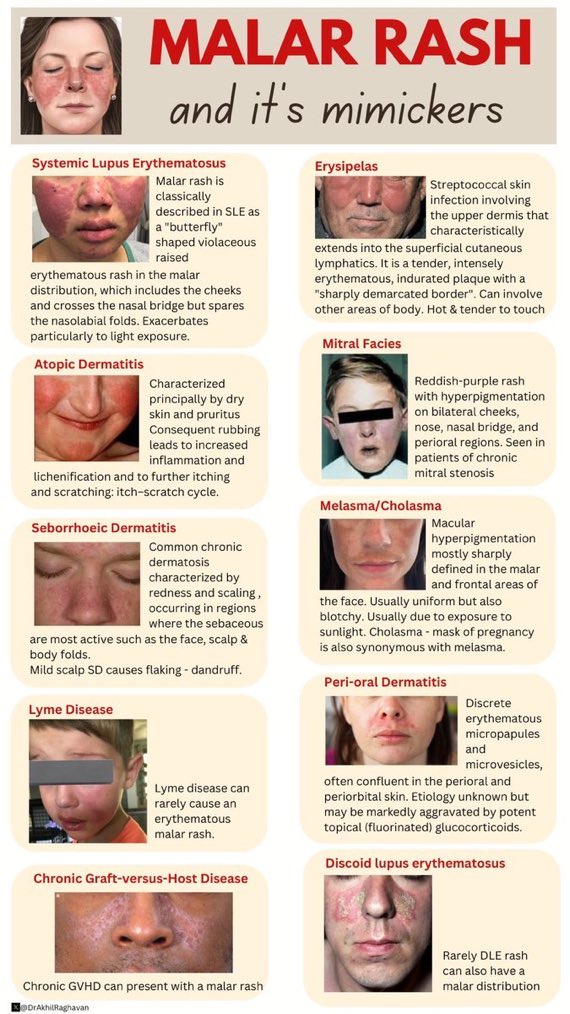
| 🌸 Systemic Lupus Erythematosus (SLE) |
- Butterfly-shaped rash across cheeks and nose (sparing nasolabial folds).
- Photosensitivity.
- Polyarthritis/arthralgia.
- Oral ulcers.
- Renal involvement (proteinuria, haematuria).
|
- ANA, Anti-dsDNA, Anti-Smith antibodies.
- FBC, renal panel, urinalysis.
- Skin biopsy if uncertain.
|
- NSAIDs for arthralgia.
- Hydroxychloroquine (mainstay).
- Steroids for flares.
- Immunosuppressants (methotrexate, azathioprine) for organ disease.
- Rigorous sun protection.
|
| 🌡️ Rosacea |
- Flushing, persistent facial erythema.
- Telangiectasia.
- Acneiform papules/pustules.
- Burning/stinging sensations.
|
- Clinical diagnosis.
- Dermatoscopy (to highlight telangiectasia).
|
- Topical metronidazole/azelaic acid.
- Oral doxycycline for moderate disease.
- Laser for telangiectasia.
- Avoid triggers (alcohol, spicy food, temperature extremes).
|
| 💜 Dermatomyositis |
- Heliotrope rash on eyelids.
- Gottron's papules on knuckles.
- Proximal muscle weakness.
- Mechanic’s hands, photosensitivity.
|
- Raised CK.
- EMG, muscle MRI.
- Muscle biopsy.
- Myositis-specific autoantibodies (Anti-Mi-2, Anti-MDA5).
|
- High-dose steroids first line.
- DMARDs: methotrexate, azathioprine.
- Screen for malignancy (paraneoplastic link).
- Physiotherapy and sun avoidance.
|
| 🧴 Seborrheic Dermatitis |
- Greasy, yellow scales on face, scalp, eyebrows.
- Mild erythema, pruritus.
- Chronic relapsing course.
|
|
- Topical antifungals (ketoconazole).
- Low-potency steroids for flares.
- Medicated shampoos (zinc pyrithione, selenium sulphide).
|
| 🌿 Allergic Contact Dermatitis |
- Itchy, erythematous rash ± vesicles/pustules.
- Often localized to allergen contact (cosmetics, metals).
|
- Patch testing.
- Careful exposure history.
|
- Avoid allergens.
- Topical steroids.
- Oral antihistamines.
- Barrier repair with emollients.
|
| 🔥 Erythroderma |
- Generalised redness/scaling ± systemic upset.
- May involve face with malar erythema.
|
- Skin biopsy.
- Full bloods, renal/liver profile.
|
- Stop offending drug.
- Emollients, topical steroids.
- Systemic immunosuppression if severe.
|
| 👁️ Periorbital Dermatitis |
- Redness and scaling around eyes.
- Often linked with steroid or cosmetic use.
|
- Clinical ± patch testing.
|
- Avoid steroids/irritants.
- Topical calcineurin inhibitors.
- Oral antihistamines for itch.
|
| 🌽 Pellagra (Niacin deficiency) |
- Dermatitis on sun-exposed skin (inc. face).
- “3 D’s”: Dermatitis, Diarrhoea, Dementia.
- Photosensitivity, scaling rash.
|
- Clinical diagnosis, dietary history.
- ± Niacin measurement.
|
- Niacin supplementation.
- High-protein, balanced diet.
|
| 🌾 Dermatitis Herpetiformis |
- Symmetrically itchy vesicles (elbows, knees, back, buttocks ± face).
- Strongly linked with coeliac disease.
|
- Skin biopsy with immunofluorescence.
- Serology: anti-tTG, anti-EMA.
|
- Strict gluten-free diet.
- Dapsone for symptom control.
|