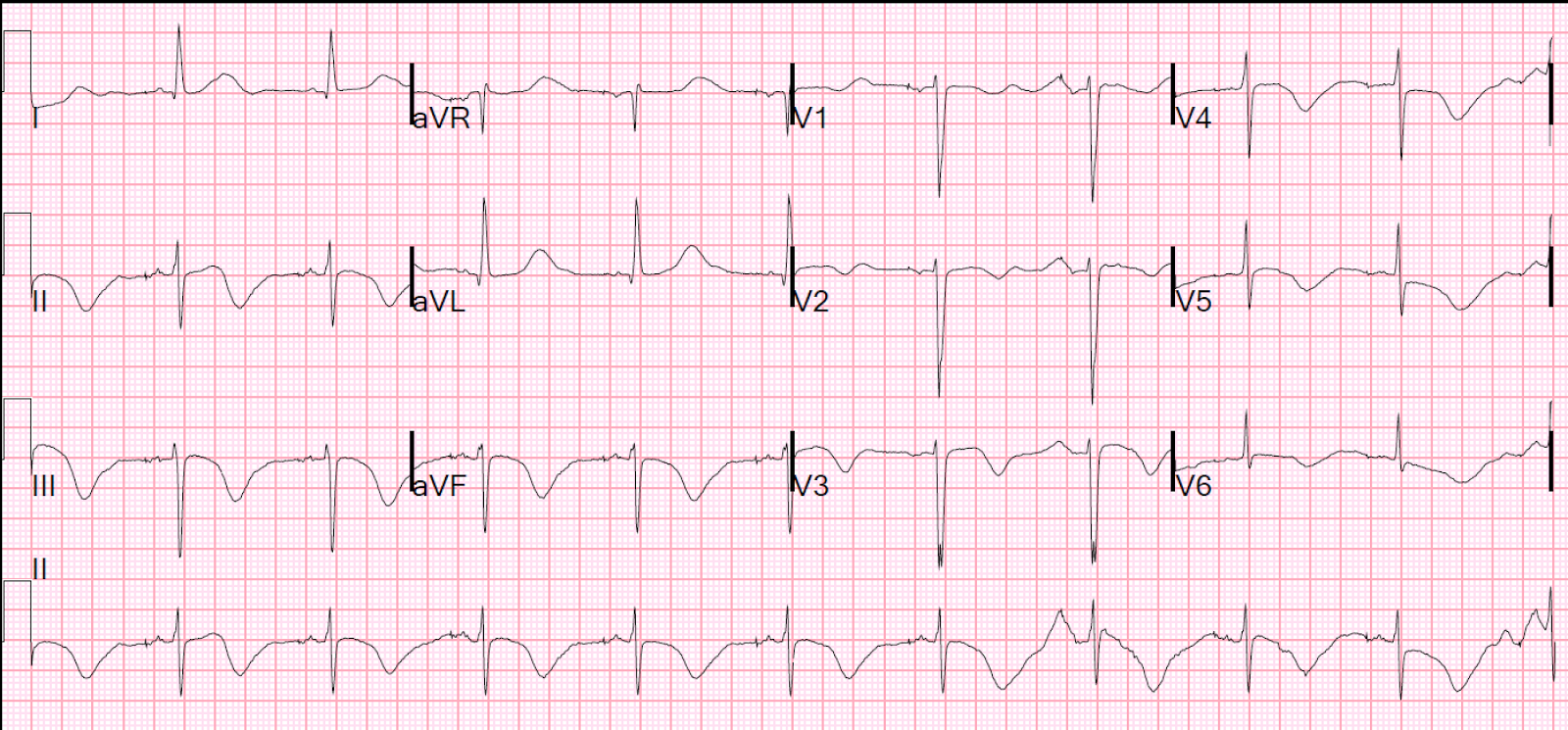
Long QT syndrome (LQTS) Congenital
Related Subjects:
|ECG-QT interval
|Brugada Syndrome
|Long QT syndrome (LQTS) Acquired
|Long QT syndrome (LQTS) Congenital
|Torsades de Pointes
|Ventricular Fibrillation
|Ventricular Tachycardia
|Resuscitation - Adult Tachycardia Algorithm
|Automatic Implantable Cardioverter Defibrillator (AICD)
⚠️ Beta blockers (BBs) reduce sympathetic stimulation of cardiac ion channels and protect against arrhythmias, particularly in LQT1 and LQT2. They are first-line therapy for most congenital LQTS patients.
📌 About Long QT Syndrome (LQTS)
- A congenital cardiac channelopathy causing prolonged QT interval and risk of Torsades de Pointes or sudden cardiac death.
- Prevalence: ~1 in 2000; often under-recognised.
⚡ Torsades de Pointes
🧬 Aetiology
- Mutations in potassium, sodium, or calcium channels → delayed ventricular repolarisation.
- QT interval prolongation = substrate for polymorphic VT (torsades) and VF.
🔑 Types
- Romano-Ward: Autosomal dominant, QT prolongation + arrhythmias.
- Jervell & Lange-Nielsen: Autosomal recessive, associated with congenital deafness + higher arrhythmic risk.
📉 Risk Factors
- Increased sympathetic tone (exercise, stress, sudden loud noises).
- Electrolyte disturbance: ↓K⁺, ↓Mg²⁺, ↓Ca²⁺.
- QT-prolonging drugs (see CredibleMeds list).
🧪 Clinical Features
- Syncope (often during exercise, swimming, or emotional stress).
- Palpitations, cardiac arrest, or sudden unexplained death in family.
- May be asymptomatic and detected on ECG screening.
📊 Diagnostic Criteria (Schwartz Score)
- QTc >480 ms = +3 points
- Torsades de Pointes = +2
- Syncope with stress = +2; without stress = +1
- Congenital deafness = +0.5
- Family history of LQTS or sudden death <30 yrs = +0.5–1
- ≥4 points = high probability of LQTS
🧪 Investigations
- ECG: QTc prolongation; repeat if borderline.
- Bloods: FBC, U&E, Ca²⁺, Mg²⁺ to exclude secondary causes.
- Genetic testing: if clinical suspicion strong.
🩺 Management
- Drug avoidance: Stop QT-prolonging drugs, avoid electrolyte disturbance.
- Beta blockers: (propranolol, nadolol, atenolol) = cornerstone, esp. in LQT1.
- ICD: For survivors of cardiac arrest, recurrent syncope despite BBs, or QTc >550 ms with high-risk features.
- LCSD (Left Cervicothoracic Sympathectomy): Considered if recurrent events despite BB therapy and ICD not suitable.
- Lifestyle advice:
- LQT1 → avoid swimming/strenuous exertion 🏊♂️
- LQT2 → avoid sudden loud noises / alarms 🔔
- All → avoid competitive sports unless risk-stratified by specialist
📚 Reference
