
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Head Injury and Traumatic Brain Head Injury (TBI)
Related Subjects: |Initial Trauma Assessment and Management |Thoracic Trauma Assessment and Management |Head Injury and Traumatic Brain Head Injury (TBI) |Flail Chest Rib fractures |Resuscitative Thoracotomy |Haemorrhage control |Traumatic Head/Brain Injury |Traumatic Cardiac Arrest |Abdominal trauma |Tranexamic Acid |Silver Trauma |Cauda Equina |Adult Resus:Basic Life Support |Adult Resus: Advanced Life Support |Resus:Acute Haemorrhage |Acute Hydrocephalus
🧠 Head injury is the most common cause of death and disability in people aged 1–40 in the UK. Refer to NICE guidance (all ages). Red flag triggers for CT: GCS < 15, LOC, focal neurology, suspected skull fracture, amnesia, persistent headache, vomiting, seizures, anticoagulant use (except aspirin alone), high-energy mechanism, or safeguarding concerns.
ℹ️ About
- 💥 Trauma to scalp, skull, or brain (excludes superficial face injuries).
- 🚗 Common causes: RTAs, falls, assaults (age & geography dependent).
- 🔒 Classified as closed (no fracture) or penetrating (with fracture).
- 📊 Accounts for ~7% of major trauma; ~5% mortality.
- ⚡ Early neuroprotective care significantly improves outcome.
Epidemiology
- 🏥 10% of A&E attendances; 25% admitted.
- Only 1% referred to neurosurgery.
- 👨 Young men highest risk; bimodal peaks in young adults and elderly.
- Head injuries = 50% of trauma deaths; 60% from RTAs.
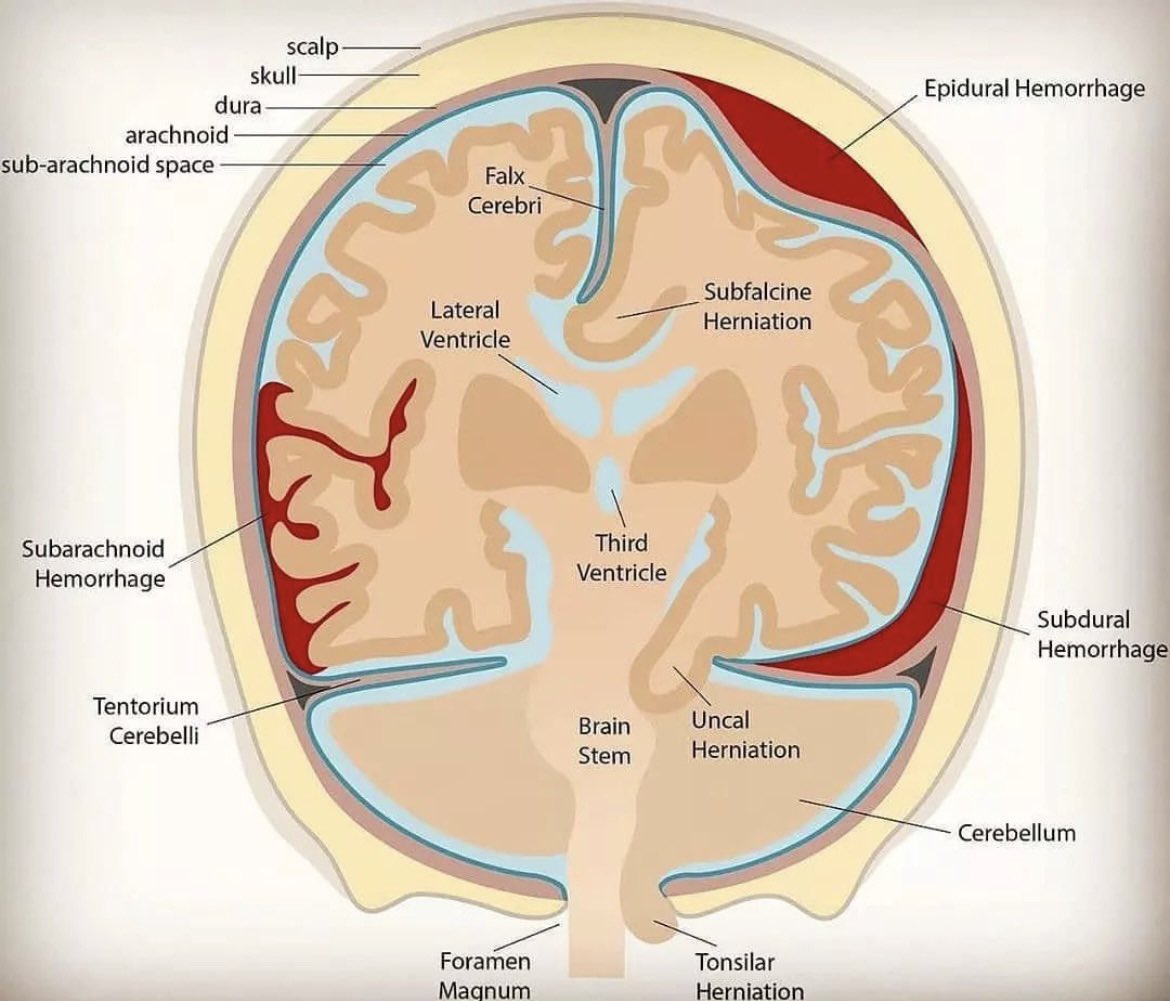
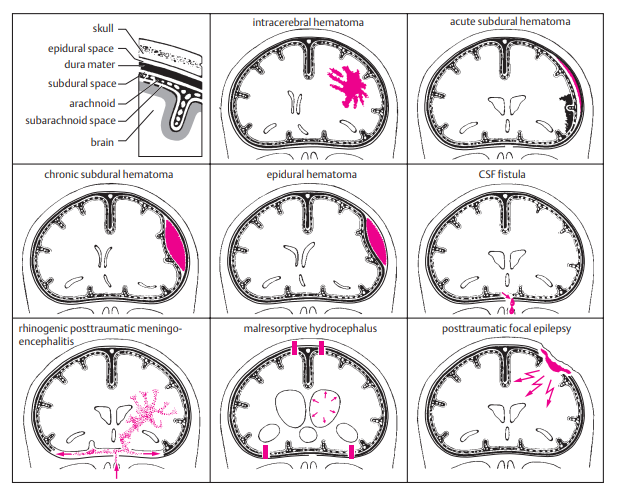
Patterns of Brain Bleeds
Mechanism of Injury
- ⚡ Direct trauma → axonal shearing, contusions, haemorrhage.
- 🧩 Primary injury: occurs at time of impact (contusions, DAI, lacerations).
- ♻️ Secondary injury: hypoxia, raised ICP, oedema, haematoma, seizures, infection.
- High-risk events: high-speed RTA, fall ≥3m, elderly fall, alcohol, altered GCS.
Risk Factors & Concerns
- 🧑🤝🧑 Groups: young men (15–29), elderly, RTAs, falls, assaults.
- By bleed type:
- 🩸 Subdural haematoma → elderly, bridging vein rupture.
- 🩸 Extradural haematoma → young, MMA rupture, lucid interval.
- 🩸 Traumatic ICH / SAH → diffuse, often with contusions.
Clinical Assessment (ABCDE + Neuro)
- 📍 Mechanism, LOC, amnesia, seizure, vomiting.
- 🧍 Full GCS & neuro exam (limbs, pupils, vision, speech).
- 👁️ Pupil dilatation + coma = brainstem compression until proven otherwise.
- 💧 CSF leak from nose/ear = base of skull fracture (check for “panda eyes” or Battle’s sign).
- 🔎 Always assess for associated trauma (C-spine, chest, long bones).
Investigations (NICE CT Criteria)
- 🕐 CT Head within 1h if:
- GCS < 13 initially or < 15 at 2h
- Open/depressed skull fracture
- Signs of base of skull fracture
- Seizure, focal deficit
- ≥1 vomiting episode
- 🕗 CT Head within 8h if:
- Age ≥ 65
- Bleeding/clotting disorder or anticoagulant/antiplatelet (except aspirin alone)
- Dangerous mechanism (ejected, fall ≥1m)
- Retrograde amnesia > 30 mins
Complications of Head Injury
| Complication | Mechanism | Clues | Management |
|---|---|---|---|
| Intracranial Haemorrhage | Arterial/venous rupture | Deteriorating GCS, focal signs | Urgent CT, craniotomy, ICP control |
| Diffuse Axonal Injury | Shearing | Low GCS, normal CT | ICU, ICP monitor, rehab |
| Skull Fractures | Linear, depressed, basilar | CSF leak, Battle’s sign, cranial nerve palsy | CT, repair if needed, meningitis prophylaxis |
| Seizures | Cortical irritability | Early or late seizures | Levetiracetam 1g BD; prophylaxis in severe |
| Cerebral Oedema | Raised ICP | Bradycardia, hypertension, irregular RR (Cushing’s) | Mannitol, hypertonic saline, hyperventilation, decompression |
| Hydrocephalus | CSF obstruction | Headache, vomiting, papilloedema | Ventriculostomy/shunt |
| PCS | Concussion | Persistent headache, poor concentration | Symptom control, neuro rehab |
| CTE | Repetitive trauma | Memory decline, behavioural change | Supportive, long-term rehab |
Infographic
💊 Management
- 🩺 ABCDE first: oxygen (SpO₂ 94–98%), 2x IV access, C-spine precautions.
- 💤 GCS ≤ 8 → intubate (call anaesthetist, RSI with neuroprotective sequence).
- 🧾 Urgent CT head/neck if indicated.
- 💉 Reverse anticoagulation (target platelets ≥100).
- 👀 Obs: GCS, pupils, vitals - half-hourly ×2h → hourly ×4h → 2-hourly if stable.
- 📌 Neurosurgical referral if: GCS ≤8, deteriorating GCS, new focal signs, abnormal CT.
- 💊 Seizure prophylaxis: Levetiracetam 1g BD IV → NG/PO when possible.
- 🤝 Long-term: early neuro-rehabilitation (OT, physio, psychology).
🌟 Exam tip: - Extradural = lucid interval, young patient, MMA tear. - Subdural = elderly, bridging veins, gradual decline. - DAI = normal CT but low GCS.
References
🧾 Clinical Case Examples
Case 1 – Extradural haematoma ⚡ A 21-year-old motorcyclist, not wearing a helmet, falls off his bike. He loses consciousness briefly, then is lucid for 1 hour before suddenly collapsing. On exam: right fixed dilated pupil, left-sided weakness. 👉 Diagnosis: Extradural haematoma (middle meningeal artery rupture). 👉 Management: Urgent CT head, neurosurgical referral for craniotomy.
Case 2 – Subdural haematoma 🩸 An 80-year-old woman on warfarin trips at home and strikes her head. Over the next 2 days she becomes confused and drowsy. GCS drops from 15 → 12. 👉 Diagnosis: Acute-on-chronic subdural haematoma (bridging vein rupture). 👉 Management: CT head, reverse anticoagulation, neurosurgical discussion.
Case 3 – Diffuse axonal injury 🧩 A 19-year-old student is involved in a high-speed RTA. At the scene his GCS is 6. In ED: intubated, CT head appears normal. 👉 Diagnosis: Diffuse axonal injury. 👉 Management: Admit to ICU, ICP monitoring, supportive neurocritical care, later rehabilitation.
Case 4 – Base of skull fracture 💧 A 35-year-old man is assaulted. He presents with periorbital bruising (“raccoon eyes”) and clear fluid leaking from the ear. 👉 Diagnosis: Basilar skull fracture with CSF leak. 👉 Management: CT head + temporal bones, neurosurgical review, prophylactic antibiotics not routinely given (unless advised by specialist), monitor for meningitis.
Case 5 – Post-concussion syndrome 🌀 A 28-year-old woman presents 2 weeks after a minor head injury. She complains of persistent headaches, poor concentration, irritability, and disturbed sleep. GCS was 15 at the time of injury, CT normal. 👉 Diagnosis: Post-concussion syndrome. 👉 Management: Reassurance, symptom control (analgesia, sleep hygiene), occupational health/psychology support if prolonged.
Case 6 – Anticoagulated head injury 💊 A 72-year-old man on apixaban falls in the bathroom, striking his head. He is GCS 15 with no focal neurology. 👉 Diagnosis: High-risk head injury on anticoagulation. 👉 Management: CT head within 1h (NICE), consider reversal if bleed, admit for observation even if initial CT normal.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery