Intraventricular haemorrhage (neonates)
🧠 Intraventricular haemorrhage (IVH) is the most common type of intracranial haemorrhage in the neonate.
It occurs primarily in preterm infants 👶 but can occasionally be seen in near-term and term babies.
📖 About
- Bleeding into the brain’s ventricles.
- Severe cases → neuronal damage and long-term brain injury 🧩.
⚙️ Aetiology
- Most common in premature babies ⏳.
- Overall incidence is falling 📉 with modern neonatal care.
- Pathogenesis: hypoxic–ischaemic reperfusion injury of the germinal matrix.
⚠️ Higher Risk Groups
- Prematurity ⏳ and very-low-birth-weight infants (<1500 g / <3 lb 5 oz)
- Respiratory distress (e.g. hyaline membrane disease) 🫁
- Complications of prematurity, labour/delivery trauma
- Maternal infection 🤰🦠, hypertension, clotting disorders
- Head injury/shaken baby 🚨
- Genetic predisposition
🔎 Clinical Features
- Apnoea, bradycardia, cyanosis 💙, poor suck
- High-pitched cry, lethargy, stupor, or coma 🛌
- Bulging/tense fontanelle 🔺
- Hypotonia, weak reflexes, seizures ⚡, decerebrate posturing
- Abnormal eye movements 👀
🧪 Investigations
- FBC: often shows anaemia 📉
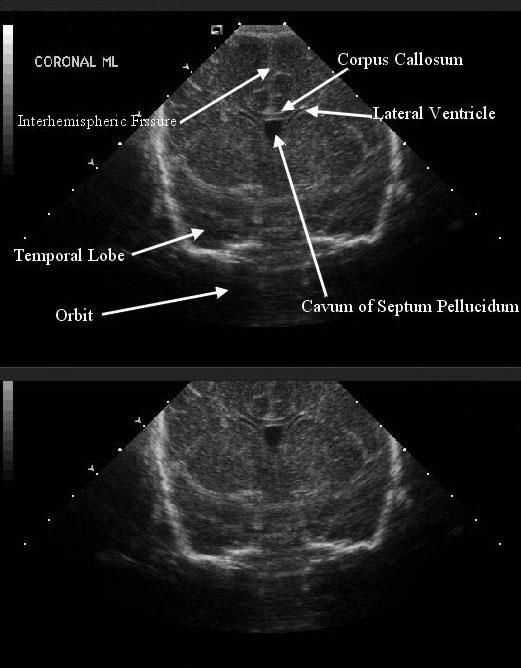
- Cranial ultrasound = diagnostic test of choice 🖥️
📊 Severity (Grading)
- Grade I: Germinal matrix only
- Grade II: Blood in ventricles
- Grade III: Ventricular dilatation
- Grade IV: Extension into parenchyma
☠️ Grades & Mortality
- Grade I: ~6% mortality
- Grade II: ~33% mortality
- Grade III: ~60% mortality
- Grade IV: ~93% mortality
💡 Exam Tip: Grade IV bleeds often cause venous infarction due to medullary venous obstruction →
secondary haemorrhage. High-yield for finals ⚡.
🩺 Management
- Prevention: Antenatal steroids (24–34 wks) reduce risk 📉.
- Screening: Premature <32 wks → routine cranial US.
- Treatment: Supportive care, ICP monitoring where indicated.
- Grades I–II: Often no long-term complications 🙂.
- Grades III–IV: Risk of hydrocephalus, neurodevelopmental delay, ↑ mortality 🚨.
📚 References
