Related Subjects:
|Brain tumour s
|Astrocytomas
|Brain Metastases
|Tuberous sclerosis
|Turcot's syndrome
|Lhermitte Duclos Disease
|Oligodendroglioma
|Acute Hydrocephalus
|Intracranial Hypertension
|Primary CNS Lymphoma (PCNSL)
Idiopathic Intracranial Hypertension (IIH), aka Pseudotumour Cerebri, is raised intracranial pressure (ICP) without structural cause.
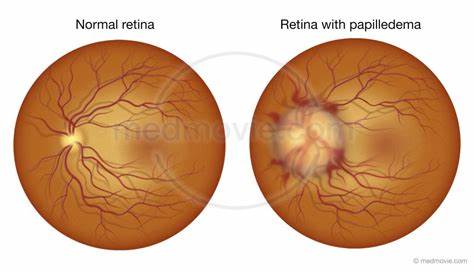
⚠️ Despite “benign” terminology, untreated IIH may cause permanent visual loss due to papilloedema.
ℹ️ Key Points
- Most common in young, obese females 📈.
- Mimics a brain tumour clinically & radiologically.
- Visual field defects: early blind spot enlargement, inferonasal loss 👁️.
🧬 Aetiology & Associations
- Impaired CSF absorption at arachnoid granulations.
- Cerebral venous sinus thrombosis must be excluded 🚨.
- Associated factors: pregnancy, OCP, thrombophilia.
- Drugs 💊: Vitamin A/retinoids, tetracyclines, growth hormone, nitrofurantoin, danazol, lithium.
- Other substances: ketamine, nitrous oxide.
🩺 Clinical Presentation
- Headache: morning-predominant, worse lying down, eased by ICP reduction.
- Visual: transient obscurations, blurred vision, papilloedema, visual field loss.
- Other: diplopia (CN VI palsy), pulsatile tinnitus, neck/back pain.
- Often history of recent weight gain ⚖️ or new medication exposure.
🔬 Investigations
- Bloods: FBC, U&E, LFT, ESR, CRP to exclude systemic causes.
- Visual field testing: blind spot enlargement, inferonasal defects.
- Imaging: MRI/MRV to exclude mass/venous thrombosis; may show empty sella, enlarged optic nerve sheath.
- LP: Elevated opening pressure (>25 cm H₂O) with normal CSF constituents.
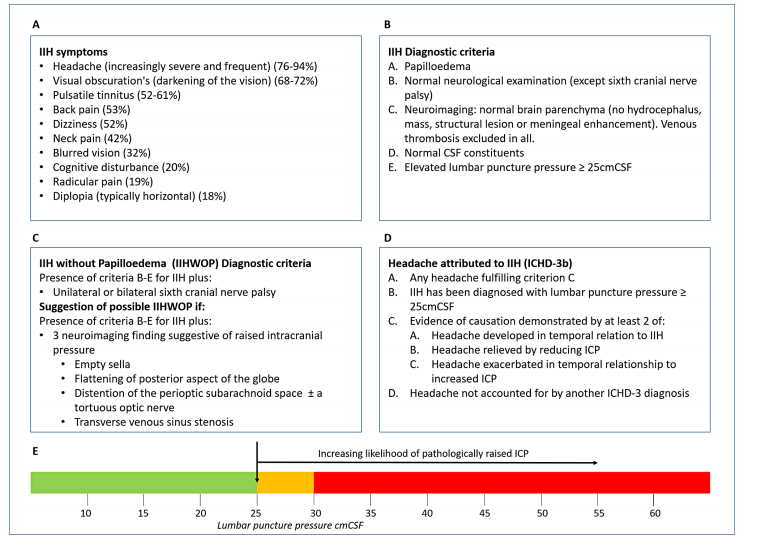
📑 Diagnostic Criteria (Modified Dandy)
- Papilloedema
- Normal neurological exam (except CN VI palsy)
- Normal imaging (no mass/structural lesion)
- Normal CSF composition
- Raised opening pressure >25 cm CSF
|
🧾 Differentials
- Cerebral venous sinus thrombosis
- Intracranial mass (tumour, abscess)
- Hydrocephalus
🎯 Management Goals
- Rule out venous sinus thrombosis.
- Preserve vision 👁️.
- Reduce ICP and control headache burden.
💊 Management
- Stop offending drugs (tetracyclines, retinoids, steroids, nitrofurantoin).
- Weight loss: 5–10% reduction lowers ICP; bariatric surgery if needed.
- Medical therapy:
- Acetazolamide – first-line, reduces CSF production.
- Topiramate – alternative, also promotes weight loss.
- Loop diuretics (e.g., furosemide) – selected cases.
- Steroids – rarely used; risk of rebound ICP on withdrawal.
- Surgical therapy:
- Optic nerve sheath fenestration – for threatened vision.
- CSF diversion (VP or LP shunt) – refractory cases.
- Venous sinus stenting – emerging therapy for stenosis-related IIH.
💡 Exam Pearls
Think “young obese woman with headache + papilloedema + raised LP opening pressure.”
👉 Always exclude venous sinus thrombosis first.
👉 First-line treatment = weight loss + acetazolamide.
📚 References & Guidelines
