
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Pituitary
Related Subjects: |AP of the Thyroid |AP of the Parathyroid |AP of the Pituitary |AP of the Pancreas |AP of the Adrenal Gland |Addisons Disease |Phaeochromocytoma |Adrenal Adenomas |Adrenal Cancer |Cushing Syndrome |Cushing Disease |Congenital Adrenal hyperplasia |Primary hyperaldosteronism (Conn's syndrome) |ACTH |McCune Albright syndrome
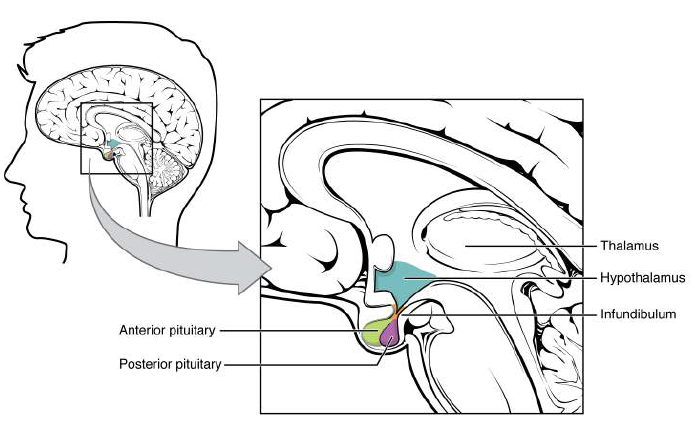
The pituitary gland (“hypophysis”) is a small endocrine organ at the base of the brain that translates hypothalamic signals into hormonal outputs controlling growth, metabolism, reproduction, lactation, stress responses, and water balance. It sits within the sella turcica of the sphenoid bone and connects to the hypothalamus via the infundibulum (pituitary stalk). Functionally, it is two glands in one: anterior pituitary (adenohypophysis) which synthesises hormones, and posterior pituitary (neurohypophysis) which stores and releases hypothalamic hormones.
📍 1) Location, Relations, and Surgical Anatomy
- Location: In the sella turcica (hypophyseal fossa) of the sphenoid bone.
- Roof: Covered by a dural fold, the diaphragma sellae, with a central opening for the pituitary stalk.
- Superior relation: Optic chiasm sits just above (clinical relevance for visual field defects).
- Lateral relations: Cavernous sinuses containing ICA and cranial nerves III, IV, V1, V2, VI.
- Inferior relation: Sphenoid sinus (route for trans-sphenoidal pituitary surgery).
📌 Clinical: Expanding pituitary macroadenoma commonly compresses the optic chiasm → bitemporal hemianopia. Cavernous sinus invasion can cause ophthalmoplegia (III/IV/VI palsies) and facial sensory symptoms (V1/V2).
🧬 2) Embryology and Development
- Anterior pituitary (adenohypophysis): develops from Rathke’s pouch (oral ectoderm) that migrates upward.
- Posterior pituitary (neurohypophysis): develops as a down-growth of the diencephalon (neuroectoderm) from the hypothalamus.
- Pars intermedia: a thin remnant between lobes (more prominent in some species; in humans may contribute small amounts of POMC-derived peptides).
📌 Clinical: Remnants of Rathke’s pouch can form a Rathke’s cleft cyst, presenting with headaches, hypopituitarism, and sometimes visual symptoms.
🏗️ 3) Microscopic Structure
🟦 Anterior Pituitary (Adenohypophysis)
- Chromophils: hormone-producing cells that stain well.
- Acidophils: somatotrophs (GH), lactotrophs (PRL).
- Basophils: corticotrophs (ACTH), thyrotrophs (TSH), gonadotrophs (FSH/LH).
- Chromophobes: less-staining cells (degranulated chromophils or supporting/stem-like cells).
🟩 Posterior Pituitary (Neurohypophysis)
- Contains axons of hypothalamic neurons (supraoptic/paraventricular nuclei) and pituicytes (glial support cells).
- Herring bodies: axonal swellings containing stored ADH/oxytocin.
🩸 4) Blood Supply and the Hypothalamo–Hypophyseal Portal System
- Superior hypophyseal artery (ICA branch) supplies the median eminence and forms a primary capillary plexus.
- Portal veins carry hypothalamic releasing/inhibiting hormones to the anterior pituitary secondary plexus.
- Inferior hypophyseal artery supplies the posterior pituitary directly.
Why a portal system? It delivers hypothalamic hormones in high concentration directly to the anterior pituitary without dilution in systemic circulation. This enables precise control with tiny amounts of releasing hormones.
📌 Clinical: The anterior pituitary is more vulnerable to hypoperfusion (portal supply) → explains Sheehan syndrome (postpartum pituitary infarction after severe haemorrhage), often presenting with failure to lactate (↓ PRL) and secondary adrenal insufficiency (↓ ACTH).
⚡ 5) Anterior Pituitary Hormones - What They Do
| Hormone | Main Target | Key Physiological Effects | High-Yield Clinical Links |
|---|---|---|---|
| GH (Growth hormone) | Liver, bone, muscle, adipose | ↑ IGF-1, linear growth, protein synthesis; ↑ lipolysis; anti-insulin effects (↑ glucose) | Excess → gigantism/acromegaly; deficiency → short stature (children), ↓ lean mass (adults) |
| PRL (Prolactin) | Breast | Milk production; suppresses GnRH (↓ fertility) | Prolactinoma, dopamine antagonists ↑ PRL; symptoms: galactorrhoea, amenorrhoea, low libido |
| ACTH | Adrenal cortex (zona fasciculata/reticularis) | ↑ cortisol (and adrenal androgens) | Excess → Cushing disease; deficiency → secondary adrenal insufficiency |
| TSH | Thyroid | ↑ T4/T3 synthesis and release; trophic growth | Secondary hypothyroidism; TSHoma (rare) → hyperthyroidism with inappropriately normal/high TSH |
| FSH | Gonads | ♀ follicle maturation + oestrogen synthesis; ♂ Sertoli cells → spermatogenesis | Hypogonadotropic hypogonadism in pituitary failure |
| LH | Gonads | ♀ ovulation + corpus luteum progesterone; ♂ Leydig cells → testosterone | Low LH/FSH → infertility, low testosterone/oestrogen |
💧 6) Posterior Pituitary Hormones - ADH and Oxytocin
🟦 ADH (Vasopressin)
- Made in: hypothalamic supraoptic nucleus (main) and paraventricular nucleus → transported down axons → released from posterior pituitary.
- Primary action: increases water reabsorption in the kidney collecting duct via V2 receptors → insertion of aquaporin-2 channels.
- V1 receptors: vasoconstriction (higher concentrations) → supports blood pressure in shock states.
- Control: plasma osmolality (osmoreceptors) + effective arterial blood volume (baroreceptors).
📌 Clinical: Central diabetes insipidus = ADH deficiency (polyuria, polydipsia, dilute urine, ↑ serum osmolality). Treat with desmopressin. Nephrogenic DI = renal resistance to ADH (e.g., lithium), treated with addressing cause ± thiazide/NSAID.
🟩 Oxytocin
- Made in: paraventricular nucleus (main) → released from posterior pituitary.
- Uterus: stimulates contractions (positive feedback during labour).
- Breast: milk let-down reflex (myoepithelial contraction) in response to suckling.
🎛️ 7) Hypothalamic Control: Releasing and Inhibiting Hormones
- TRH → ↑ TSH (and can ↑ prolactin)
- CRH → ↑ ACTH
- GnRH (pulsatile) → ↑ LH/FSH (continuous GnRH suppresses)
- GHRH → ↑ GH
- Somatostatin → ↓ GH (and ↓ TSH)
- Dopamine → ↓ prolactin (tonic inhibition)
Feedback loops stabilise the system: cortisol suppresses CRH/ACTH; T3/T4 suppress TRH/TSH; IGF-1 suppresses GH (and GHRH).
⚙️ 8) Key Integrated Physiology (High-Yield Mechanisms)
- Stress axis (HPA): CRH → ACTH → cortisol. Cortisol maintains vascular tone, supports gluconeogenesis, modulates immunity.
- Thyroid axis (HPT): TRH → TSH → T4/T3. Thyroid hormones increase basal metabolic rate and potentiate catecholamines.
- Gonadal axis (HPG): pulsatile GnRH → LH/FSH → sex steroids + gametogenesis.
- Growth axis: GHRH/somatostatin balance → GH → IGF-1. GH is pulsatile (peaks during sleep) and rises with exercise and fasting.
- Water balance: ADH responds to osmolality first, then volume/pressure; small increases in osmolality cause meaningful ADH release.
🚨 9) Clinical Relevance (Common Presentations)
🎗️ Pituitary Adenomas
- Microadenoma: <10 mm; Macroadenoma: ≥10 mm.
- Mass effects: headache, bitemporal hemianopia, cranial nerve palsies (cavernous sinus).
- Hormone effects:
- Prolactinoma (most common): galactorrhoea, amenorrhoea, infertility, low libido/ED. Treat with cabergoline or bromocriptine.
- GH adenoma: acromegaly (hands/feet/jaw enlargement, diabetes, OSA, cardiomyopathy). Diagnose with ↑ IGF-1 and GH not suppressing on OGTT.
- ACTH adenoma: Cushing disease (central obesity, proximal myopathy, bruising, hypertension, glucose intolerance).
🧨 Pituitary Apoplexy
- Acute haemorrhage/infarction of pituitary tumour → sudden severe headache, vomiting, visual loss, ophthalmoplegia, collapse.
- Emergency: steroids (treat potential adrenal crisis) + urgent endocrine/neurosurgical input.
⬇️ Hypopituitarism
- Causes: tumours, surgery/radiotherapy, apoplexy, Sheehan syndrome, infiltrative disease.
- Pattern often begins with: ↓ GH/↓ gonadotrophins, then ↓ TSH, and finally ↓ ACTH (life-threatening if missed).
💧 SIADH vs Diabetes Insipidus
- SIADH: excess ADH → water retention → hyponatraemia with inappropriately concentrated urine.
- DI: absent/ineffective ADH → dilute urine + hypernatraemia risk if intake inadequate.
🧪 10) Practical Investigation Summary
- Baseline labs: 9am cortisol, TSH + free T4, prolactin, IGF-1, LH/FSH + testosterone/oestradiol, electrolytes (Na+).
- Dynamic tests: OGTT for GH suppression; short synacthen (for adrenal axis) depending on scenario.
- Imaging: Pituitary MRI with contrast for adenomas and stalk lesions.
- Visual assessment: Formal visual fields if macroadenoma suspected.
📝 Summary
The pituitary gland is a central endocrine integrator linking the hypothalamus to peripheral endocrine organs. The anterior pituitary synthesises GH, PRL, ACTH, TSH, LH and FSH under hypothalamic portal control, while the posterior pituitary stores and releases hypothalamic ADH and oxytocin. Clinical disease arises from hormone excess (commonly adenomas), hormone deficiency (hypopituitarism), or posterior pituitary dysregulation (SIADH/DI), and mass effects can threaten vision and cranial nerve function.
📌 Exam Pearls
- Prolactinoma is the commonest pituitary adenoma; dopamine inhibits prolactin (dopamine antagonists ↑ PRL).
- Bitemporal hemianopia suggests optic chiasm compression by macroadenoma.
- Sheehan syndrome follows postpartum haemorrhage; failure to lactate is a classic early clue.
- Central DI responds to desmopressin; nephrogenic DI does not.
- Always consider secondary adrenal insufficiency in pituitary disease - it can be life-threatening.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery