
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Haemorrhagic stroke
Related Subjects: |Subarachnoid Haemorrhage |Perimesencephalic Subarachnoid haemorrhage |Haemorrhagic stroke |Cerebellar Haemorrhage |Putaminal Haemorrhage |Thalamic Haemorrhage |ICH Classification and Severity Scores |Acute Hydrocephalus
🧠 Introduction
- Haemorrhagic stroke, also called Spontaneous Intracerebral Haemorrhage (SICH), is often sudden and devastating.
- Accounts for ~15% of all strokes (majority are ischaemic).
- One subtype is Subarachnoid Haemorrhage (SAH), usually from ruptured aneurysms or vascular anomalies (discussed separately).
- ⚠️ Mortality is high: 30–50% of patients with large bleeds die within 30 days.
- Smaller bleeds can have better outcomes → focus on identifying cause and preventing recurrence.
- ❌ Traumatic intracranial haemorrhage and extra-axial bleeds (subdural, extradural) are not classified as stroke.
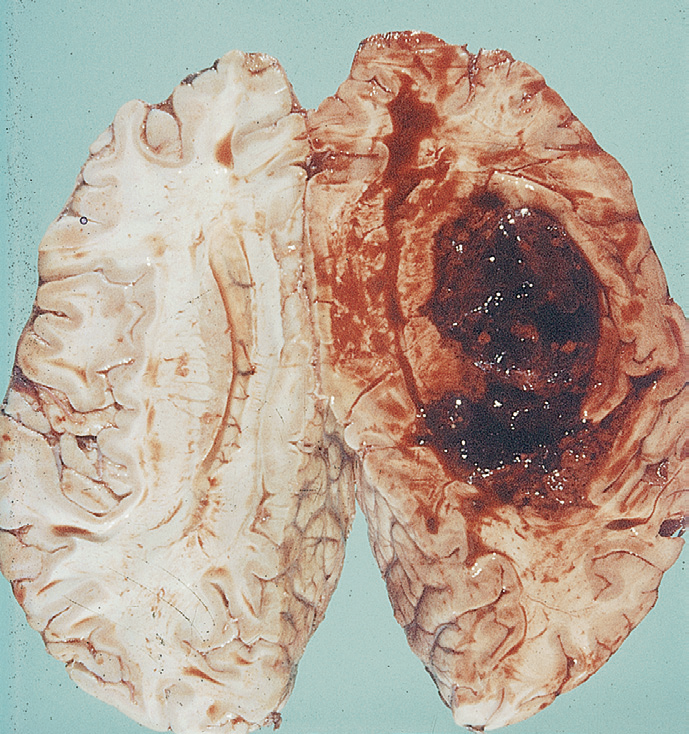
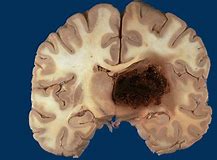
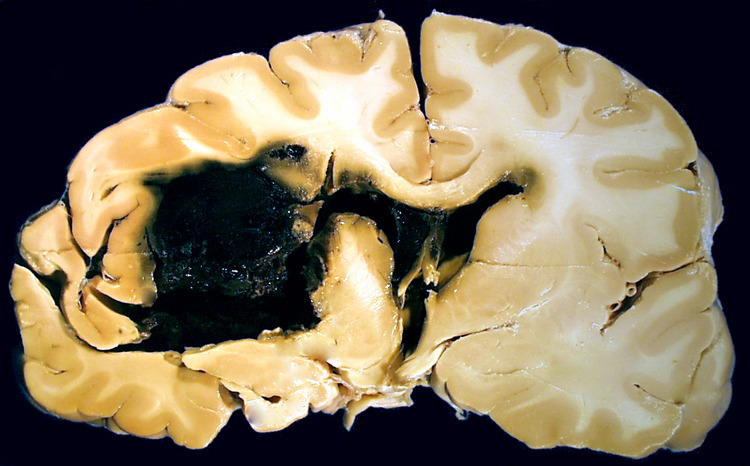
🔬 Pathological Appearance
On pathology and imaging, haemorrhagic strokes show destructive haematomas, surrounding oedema, and pressure effects:
⚙️ Aetiology
- Vessel rupture: Can occur anywhere from Circle of Willis arteries to small penetrating arterioles, capillaries, and draining veins.
- Aneurysms: Berry aneurysm rupture → high-pressure SAH.
- Small vessel disease: Hypertension → lipohyalinosis, Charcot–Bouchard microaneurysms → deep bleeds.
- Cerebral amyloid angiopathy: In elderly → lobar bleeds.
- Structural: AVMs, cavernomas, hereditary haemorrhagic telangiectasia.
- Neoplastic: Tumours (esp. melanoma, RCC, thyroid, choriocarcinoma, lung) prone to bleed.
- Coagulopathies: Anticoagulants (warfarin, DOACs), antiplatelets, thrombocytopenia, haemophilia, liver disease.
- Venous sinus thrombosis: Back-pressure haemorrhage → paradoxically requires anticoagulation.
🌍 Epidemiology
- More common in Afro-Caribbean, South-East Asian, and Japanese populations.
- Strong association with hypertension prevalence and genetic predisposition (amyloid angiopathy).
🧾 Causes by Age Group
- 🧓 Elderly: Hypertension, cerebral amyloid angiopathy.
- 👩 Younger adults: AVMs, aneurysms, cavernomas, coagulopathies.
- 💊 Any age: Anticoagulation therapy, illicit drugs (cocaine, amphetamines).
🧭 Types by Anatomy
- 🧠 Lobar: Cortex ± subcortical white matter.
- ⚫ Deep: Putaminal, thalamic, caudate, basal ganglia.
- 🧩 Brainstem: Pontine haemorrhage → sudden coma, pinpoint pupils.
- 🌀 Cerebellar: Ataxia, vertigo; large bleeds (>3 cm) may need evacuation.
- 💥 Subarachnoid haemorrhage: Usually aneurysmal.
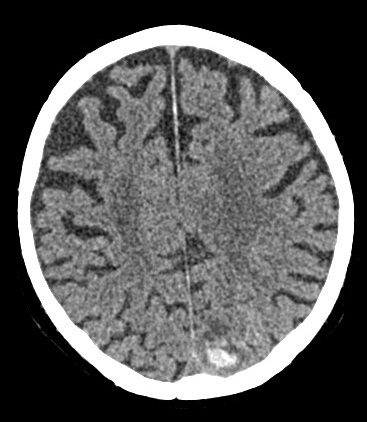
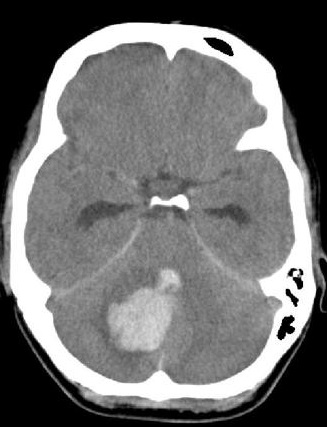
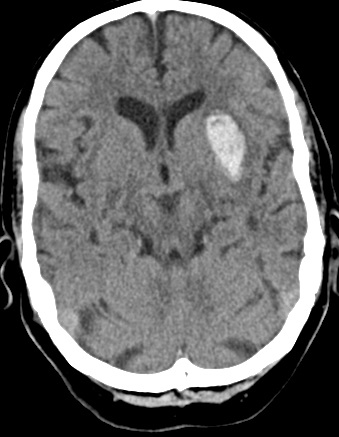
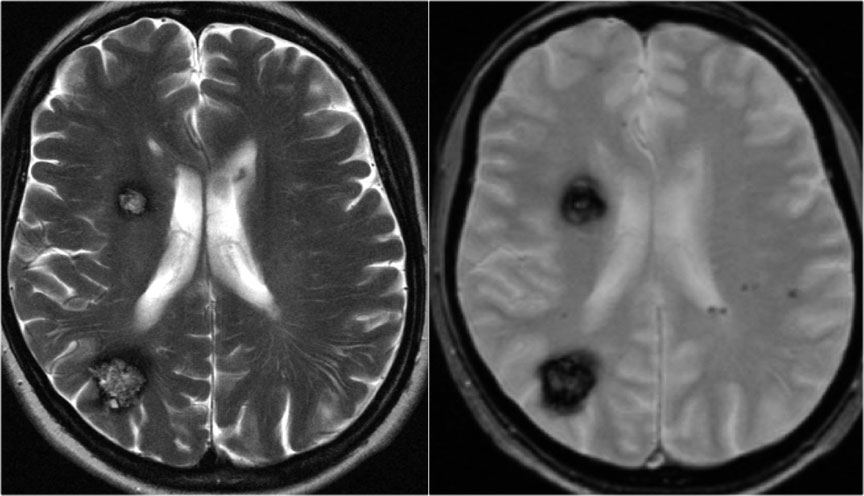
📸 Example Imaging
CT and MRI examples of haemorrhagic stroke:




🩺 Clinical Presentation
- 🧨 Sudden severe headache, vomiting, reduced consciousness.
- 🧑⚕️ Focal neurology: hemiparesis, hemisensory loss, aphasia, neglect, visual field deficits.
- 🌀 Cerebellar bleeds: vertigo, nausea, truncal ataxia, nystagmus.
- 🟣 Brainstem bleeds: coma, quadriplegia, miosis, “locked-in” syndrome.
- 🔦 SAH: Thunderclap headache, collapse, meningism, reduced GCS.
⚠️ Complications
- Intraventricular extension → acute deterioration, coma.
- Hydrocephalus from ventricular obstruction.
- Cerebral oedema, raised ICP, herniation (coning).
- Seizures (early or delayed).
- Rebleeding, especially in aneurysmal SAH and AVM.
🚩 Red Flags for Secondary Causes
- Age <50.
- No history of hypertension.
- Recurrent or atypical bleeds.
- Lobar location (esp. with soft tissue swelling or fracture → trauma vs primary bleed).
- Family history or features of inherited vascular syndromes (HHT).
🔍 Investigations
- 🩸 Bloods: FBC, U&E, LFT, glucose, coagulation, ESR/CRP.
- 🖼️ Non-contrast CT: First-line, detects haematoma, intraventricular blood, hydrocephalus.
- 🧲 MRI: Detects microbleeds, chronic haemosiderin, cavernomas (SWI/GRE).
- 📡 MRA/CTA: Aneurysms, AVMs, dissections.
- 🩻 MRV: Suspected venous sinus thrombosis.
- 📌 DSA: Gold standard for vascular malformations; small stroke risk.
- ❤️ Echocardiography: Endocarditis, embolic source.
- 💉 LP: For SAH if CT normal but suspicion high.
📊 Prognostic Scoring (ICH Score)
- GCS: 3–4 (+2), 5–12 (+1), 13–15 (0).
- Age ≥80: +1.
- Volume >30 ml: +1.
- Intraventricular haemorrhage: +1.
- Infratentorial location: +1.
➡️ Higher total = worse prognosis. 0 = 0%, 1 = 13%, 2 = 26%, 3 = 72%, 4 = 97%, 5 = 100% 30-day mortality.
⚖️ Management
- 🛑 Immediate: ABC, airway support, early CT, correct coagulopathy, cautious BP lowering, neurosurgical referral.
- 💊 Reverse anticoagulation: Warfarin INR>1.4 → Vit K + PCC (Octaplex). Stop DOAC/antiplatelets. Avoid platelets (PATCH trial).
- 📉 Blood pressure: Reduce to <160 systolic with IV agents (e.g. labetalol). Avoid hypoperfusion.
- 🧑⚕️ Neurosurgery: Consider clot evacuation, especially cerebellar bleeds >3 cm or deteriorating GCS. EVD for hydrocephalus.
- 💉 Seizure control: IV phenytoin/levetiracetam if seizures.
- 🧑🦽 Rehabilitation: MDT stroke/ICU team for survivors.
- ❌ Avoid: Routine mannitol (except bridging), steroids (harmful), unnecessary statin withdrawal without review.
📉 Prognosis
- Large bleeds, IVH, infratentorial location, and advanced age = worse outcomes.
- Many survivors are left with major neurological deficits.
💡 Exam Pearl: Intracerebral haemorrhage = sudden headache + neuro deficit + ↓ consciousness. ➡️ Early non-contrast CT is essential - clinical features alone cannot distinguish from ischaemic stroke.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery