
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Colposcopy
Related Subjects: |Causes of abnormal Vaginal bleeding |Vaginal Carcinoma |Cervical cancer |Endometrial (Uterine) Cancer |Post Menopausal Bleeding |Anatomy of the Uterus |Anatomy of the Ovary |Gynaecological History Taking |Colposcopy |Premature Menopause |Polycystic Ovary syndrome
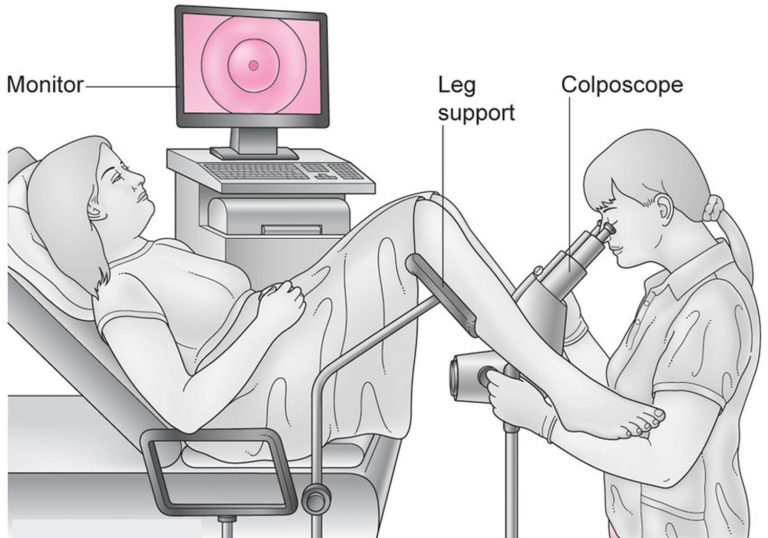
🔎 Colposcopy is a specialist examination used to assess the cervix, and sometimes the vagina or vulva, using magnification and a strong light source. In UK practice it is most commonly performed after an abnormal cervical screening result, usually when high-risk HPV (hrHPV) is found together with cytological abnormalities, or after certain persistent abnormal screening pathways. It helps identify abnormal epithelium, guide targeted biopsy, and in some cases allows immediate treatment of cervical intraepithelial neoplasia (CIN).
📖 About
- Colposcopy is usually performed in an outpatient clinic.
- A colposcope stays outside the body; it does not enter the vagina.
- The purpose is to inspect the transformation zone, where most cervical precancerous change arises.
- It is a diagnostic assessment; biopsy may be taken if needed.
- Most people referred to colposcopy do not have cervical cancer.
Indications
- Abnormal cervical screening pathway: most commonly after hrHPV-positive screening with abnormal cytology.
- Persistent hrHPV-related abnormalities or surveillance after previous CIN treatment, according to programme pathways.
- Persistent inadequate screening results in some pathway-defined situations.
- Visible abnormality of the cervix, vagina, or vulva.
- Symptoms or signs that raise concern for cervical pathology, for example unexplained postcoital bleeding or suspicious cervical appearance.
Equipment
- Colposcope: binocular magnifying instrument with illumination.
- Speculum: to visualise the cervix.
- 3–5% acetic acid: highlights abnormal epithelium by causing acetowhitening.
- Lugol’s iodine: sometimes used to help define abnormal areas.
- Biopsy forceps: for directed cervical biopsy.
- Treatment equipment may also be available in see-and-treat settings.
A trained colposcopist performs the examination, usually with an assistant and appropriate chaperoning in line with local policy.
Procedure
- Preparation: explain the procedure, obtain consent, and position the patient for speculum examination.
- Speculum examination: the cervix is exposed and inspected.
- Identify the transformation zone: assess whether it is fully visible and look for any abnormal area.
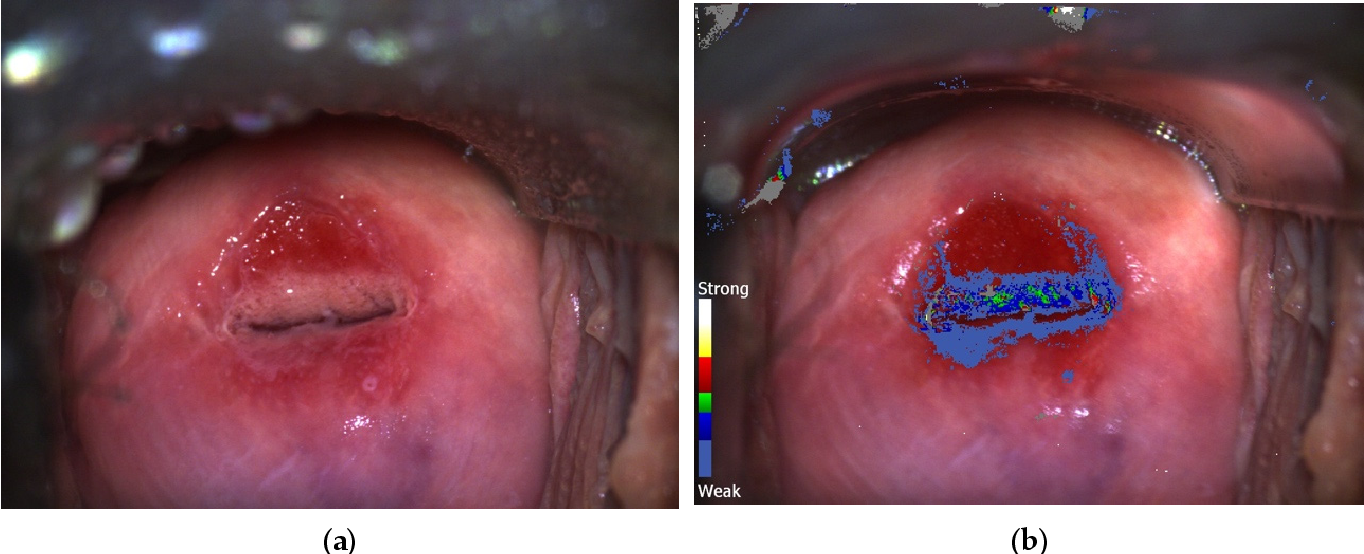
- Apply acetic acid: abnormal epithelium may turn white (acetowhite change).
- Assess vascular and surface patterns: punctuation, mosaicism, atypical vessels, lesion margins, and extent are noted.
- Optional iodine application: may help define glycogen-poor abnormal areas.
- Targeted biopsy: taken from suspicious areas if indicated.
- Management plan: follow-up, surveillance, or treatment depends on findings and histology.
What colposcopy looks for
- Acetowhite epithelium.
- Punctuation and mosaic vascular patterns.
- Atypical vessels, which may suggest higher-grade disease or malignancy.
- The location and extent of the lesion within the transformation zone.
Biopsy and histology
- Biopsy is usually targeted to the most abnormal area.
- Histology may show CIN1, CIN2, CIN3, glandular abnormality, or invasive malignancy.
- Management decisions are based on the combination of screening result, colposcopic impression, and histology.
Complications and limitations
- Usually well tolerated, but can cause discomfort, light bleeding, or vasovagal symptoms.
- Biopsy may cause a small amount of bleeding.
- Infection is uncommon.
- Accuracy depends on visibility of the transformation zone and operator experience.
- There is some interobserver variability, which is why training and quality assurance matter.
Follow-up and management
- Normal or low-risk findings: follow the relevant screening or surveillance pathway.
- Low-grade lesions: may be observed or followed up according to programme guidance.
- High-grade lesions: often require treatment, commonly by LLETZ (large loop excision of the transformation zone).
- Glandular abnormalities or suspected malignancy need specialist management.
- After treatment, patients usually enter a defined test-of-cure / surveillance pathway.
Key UK points
- UK screening is based on primary hrHPV testing.
- Colposcopy referral is commonly triggered by hrHPV positivity with abnormal cytology.
- Most referrals are for precancerous change, not invasive cancer.
- Colposcopy helps prevent cervical cancer by identifying and treating CIN before invasion occurs.
Conclusion
Colposcopy is central to the UK cervical screening pathway. It allows careful assessment of the cervix after an abnormal screening result, helps identify HPV-related epithelial change, and guides biopsy or treatment where needed. Good colposcopy depends on clear visualisation of the transformation zone, accurate recognition of abnormal patterns, and integration of findings with histology and the national screening pathway.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery