⚡ Emergency Red Flag: A sudden thunderclap headache reaching maximal intensity within minutes must be treated as a possible subarachnoid haemorrhage (SAH).
Urgent CT brain and specialist referral are required. Mortality remains high (~30–40%), but early aneurysm occlusion significantly improves outcomes.
| 🚑 Immediate Management of Suspected SAH |
|---|
- ABCDE assessment; provide oxygen and airway support if reduced consciousness.
- Urgent CT brain (non-contrast) to confirm haemorrhage.
- CT angiography to identify aneurysm if SAH confirmed.
- Blood pressure control: usually aim SBP <160 mmHg prior to aneurysm securing.
- Nimodipine 60 mg orally/NG every 4 hours for 21 days to reduce risk of delayed cerebral ischaemia.
- Reverse anticoagulation promptly if patient is anticoagulated.
- Early neurosurgical or neurointerventional referral for aneurysm occlusion.
- Definitive treatment: endovascular coiling or surgical clipping.
|
🧠 Definition
- Subarachnoid haemorrhage is bleeding into the subarachnoid space between the arachnoid and pia mater.
- Blood mixes with cerebrospinal fluid and spreads rapidly through basal cisterns, sulci, and ventricles.
- Most cases are due to rupture of a saccular (berry) aneurysm arising from the circle of Willis.
📊 Epidemiology
- Incidence: ~6–9 per 100,000 people per year.
- Peak age: 40–60 years.
- Approximately 1–2% of adults harbour unruptured intracranial aneurysms.
- Mortality ~30–40%; many survivors have long-term neurological disability.
🧬 Pathophysiology
- Intracranial aneurysms arise due to weakening of the arterial wall.
- Histology shows degeneration of the internal elastic lamina and thinning of the tunica media.
- Haemodynamic stress at arterial bifurcations leads to progressive aneurysm enlargement.
- Rupture allows arterial blood to rapidly enter the subarachnoid space causing:
- Sudden increase in intracranial pressure
- Meningeal irritation
- Global cerebral hypoperfusion
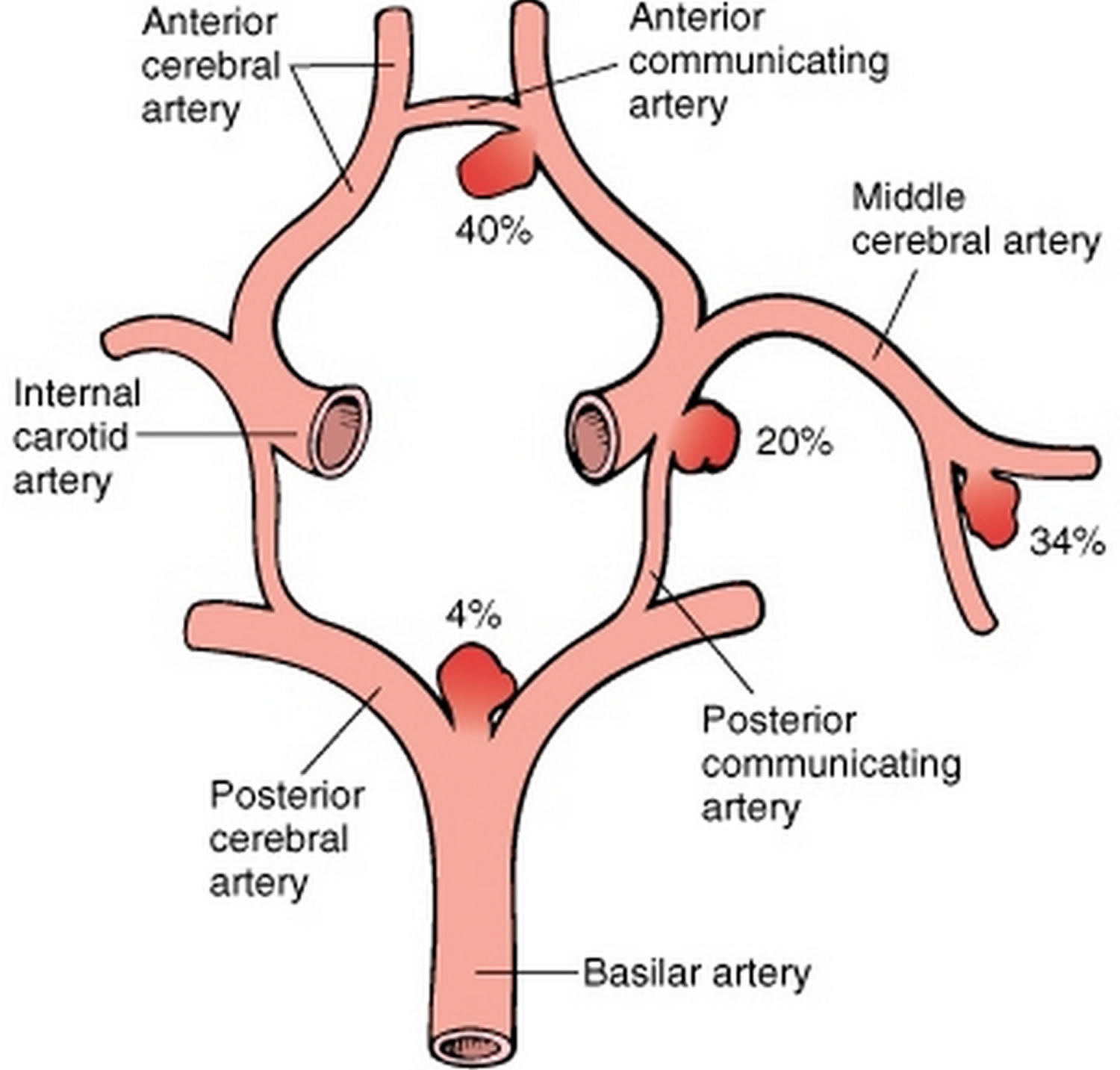
🧠 Common Aneurysm Locations
| Location |
Approximate Frequency |
| Anterior communicating artery |
~35% |
| Posterior communicating artery |
~30% |
| Middle cerebral artery bifurcation |
~20% |
| Basilar tip |
~5% |
⚠️ Risk Factors for Aneurysm Formation and Rupture
- Smoking
- Hypertension
- Excess alcohol
- Stimulant drugs (e.g. cocaine)
- Autosomal dominant polycystic kidney disease
- Ehlers–Danlos syndrome
- Marfan syndrome
🩺 Clinical Presentation
- Sudden thunderclap headache (“worst headache of life”).
- Nausea and vomiting.
- Neck stiffness and photophobia.
- Reduced consciousness.
- Focal neurological deficits.
- Seizures may occur.
🖼️ CT Imaging – Subarachnoid Haemorrhage
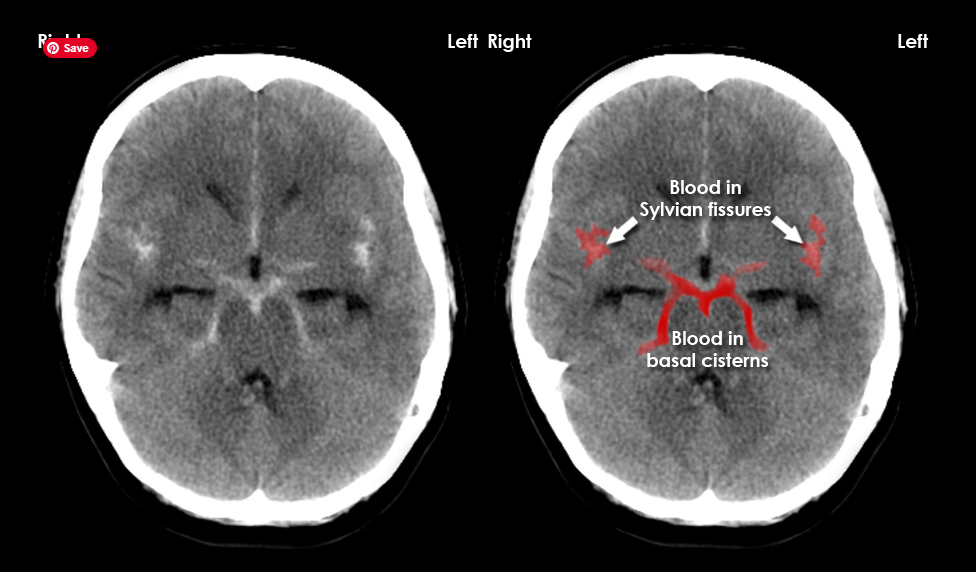

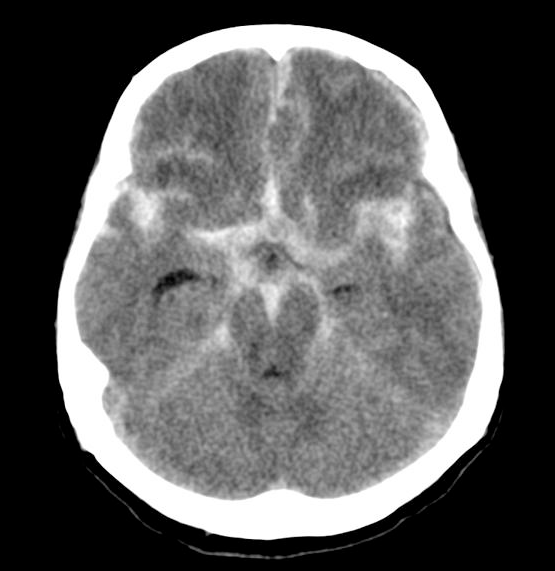
Acute blood appears hyperdense (white) within the normally dark CSF spaces.
Common locations include the basal cisterns, sylvian fissures, and cortical sulci.
🔍 Diagnostic Pathway
- Non-contrast CT brain is the first-line investigation.
- Sensitivity ~95–99% within 6 hours of symptom onset.
- If CT is negative but clinical suspicion remains high → perform lumbar puncture after 6 hours.
- Lumbar puncture looks for xanthochromia caused by haemoglobin breakdown.
- CT angiography or MR angiography is used to identify aneurysms.
- Digital subtraction angiography remains the gold standard for vascular imaging.
📊 Clinical Severity Grading
Hunt–Hess Scale
| Grade |
Clinical Features |
| I |
Mild headache |
| II |
Severe headache and neck stiffness |
| III |
Drowsiness or mild focal deficit |
| IV |
Stupor with neurological deficit |
| V |
Deep coma |
Fisher CT Scale
| Grade |
CT Findings |
| 1 |
No blood detected |
| 2 |
Diffuse thin SAH |
| 3 |
Thick clot (>1 mm) |
| 4 |
SAH with intraventricular haemorrhage |
🖥️ CT Findings in Subarachnoid Haemorrhage
Non-contrast CT head is the first-line investigation for suspected subarachnoid haemorrhage (SAH).
Acute blood appears hyperdense (bright white) relative to cerebrospinal fluid because haemoglobin has higher X-ray attenuation.
Typical CT Appearance
- Hyperdense blood in subarachnoid spaces
- Blood commonly collects in:
- Basal cisterns
- Sylvian fissures
- Interhemispheric fissure
- Cortical sulci
- In severe haemorrhage, blood may extend into the ventricular system causing intraventricular haemorrhage.
Characteristic Patterns
| CT Pattern |
Clinical Significance |
| Blood in basal cisterns |
Typical of aneurysmal SAH |
| Blood in sylvian fissures |
Often associated with MCA aneurysm rupture |
| Interhemispheric fissure blood |
Suggests anterior communicating artery aneurysm |
| Perimesencephalic blood |
Usually benign non-aneurysmal SAH |
| Convexity SAH |
Often traumatic or due to reversible cerebral vasoconstriction syndrome |
CT Sensitivity Over Time
| Time from Headache Onset |
Approximate CT Sensitivity |
| < 6 hours |
95–99% |
| 24 hours |
~90% |
| 3 days |
~75% |
| 1 week |
~50% |
Sensitivity decreases over time because blood becomes diluted and broken down within cerebrospinal fluid.
If CT is negative but clinical suspicion remains high, lumbar puncture is recommended to detect xanthochromia.
Secondary Findings on CT
- Hydrocephalus – enlarged ventricles due to obstruction of CSF circulation.
- Intraventricular haemorrhage – blood within lateral or third ventricles.
- Cerebral oedema – loss of grey–white differentiation.
- Early infarction due to vasospasm.
🔎 Key diagnostic clue: Blood within the basal cisterns around the Circle of Willis strongly suggests rupture of an intracranial aneurysm.
⚠️ Major Complications
- Re-bleeding – highest risk in first 24 hours.
- Delayed cerebral ischaemia due to vasospasm (days 3–14).
- Hydrocephalus from impaired CSF circulation.
- Seizures.
- Hyponatraemia due to SIADH or cerebral salt wasting.
Xanthochromia "Yellow Colour" of CSF

🚑 Acute Management of Subarachnoid Haemorrhage
- Immediate ABCDE Assessment
- Assess airway, breathing, circulation, disability, and exposure.
- Give supplemental oxygen to maintain adequate oxygen saturation.
- Secure airway if reduced consciousness (e.g. GCS ≤8).
- Early involvement of critical care if airway or ventilation is compromised.
- Urgent Neuroimaging
- Non-contrast CT head is the first-line investigation.
- If CT confirms subarachnoid haemorrhage, perform CT angiography to identify an aneurysm.
- If CT is negative but suspicion remains high, perform lumbar puncture ≥6 hours after headache onset to detect xanthochromia.
- Blood Pressure Management
- Aim systolic blood pressure approximately 140–160 mmHg prior to aneurysm repair.
- Avoid severe hypertension which increases risk of re-bleeding.
- Use IV antihypertensive agents if required (e.g. labetalol).
- Avoid hypotension as this may worsen cerebral perfusion.
- Nimodipine Therapy
- Start nimodipine 60 mg orally or via NG tube every 4 hours.
- Continue for 21 days.
- Reduces the risk of delayed cerebral ischaemia caused by vasospasm.
- Fluid and Electrolyte Management
- Maintain euvolaemia with isotonic fluids.
- Avoid dehydration and hypotonic solutions.
- Monitor sodium closely because hyponatraemia is common (SIADH or cerebral salt wasting).
- Reversal of Anticoagulation
- Reverse warfarin with vitamin K and prothrombin complex concentrate.
- Use specific reversal agents for DOACs where indicated.
- Stop antiplatelet agents where clinically appropriate.
- Pain and Agitation Control
- Treat severe headache with appropriate analgesia.
- Avoid excessive sedation that could obscure neurological assessment.
- Control agitation to prevent blood pressure spikes.
- Seizure Management
- Treat seizures promptly with anticonvulsants (commonly levetiracetam).
- Routine prophylactic anticonvulsants are not usually required.
- Monitoring for Hydrocephalus
- Watch for deteriorating consciousness or new neurological deficits.
- Repeat CT imaging if clinical deterioration occurs.
- External ventricular drainage may be required if hydrocephalus develops.
- Definitive Aneurysm Treatment
- Early occlusion of the aneurysm prevents re-bleeding.
- Endovascular coiling is the most common treatment in modern UK practice.
- Surgical clipping may be used depending on aneurysm anatomy.
- Ideally performed within 24–72 hours.
- Transfer to Specialist Neuroscience Centre
- Early referral to neurosurgery or interventional neuroradiology.
- Most patients require management in a neuro-ICU or specialist stroke unit.
⚠️ The highest risk of re-bleeding occurs within the first 24 hours before the aneurysm is secured. Early stabilisation, blood pressure control, nimodipine therapy, and urgent neurosurgical management are therefore essential priorities.
⚠️ Early Complications Requiring Monitoring
- Re-bleeding – highest risk within the first 24 hours.
- Delayed cerebral ischaemia due to vasospasm (days 3–14).
- Hydrocephalus causing reduced consciousness.
- Hyponatraemia due to SIADH or cerebral salt wasting.
Key priorities in the first 24 hours are blood pressure control, prevention of re-bleeding, nimodipine therapy, and urgent aneurysm occlusion.
🧠 Definitive Aneurysm Treatment
- Endovascular coiling – catheter-based insertion of platinum coils into aneurysm.
- Surgical clipping – neurosurgical placement of clip across aneurysm neck.
- Most UK centres now favour endovascular coiling when anatomically suitable.
- Treatment ideally occurs within 24–72 hours to prevent re-bleeding.
🏥 Definitive Aneurysm Treatment: Clipping vs Coiling
| Intervention |
Pros ✅ |
Cons ⚠️ |
| Surgical Clipping |
- Definitive closure of aneurysm with low recurrence rate.
- Allows direct visualisation of aneurysm and surrounding vessels.
- Good for complex aneurysms not suitable for coiling (broad neck, fusiform).
- Can simultaneously treat associated intracerebral haematoma if present.
|
- Requires craniotomy → more invasive.
- Higher risk of perioperative complications (infection, stroke, seizures).
- Longer ICU/hospital stay compared to coiling.
- Not ideal for elderly or comorbid patients.
|
| Endovascular Coiling |
- Minimally invasive (via femoral or radial artery access).
- Shorter recovery, less pain, lower initial morbidity and mortality in some studies.
- Preferred in elderly or high surgical risk patients.
- Good for aneurysms accessible via endovascular route (narrow neck or favorable dome/neck ratio).
|
- Higher long-term recurrence/need for retreatment compared to clipping.
- Cannot treat associated intracerebral haematoma directly.
- Procedure may fail if aneurysm anatomy is complex (wide neck, tortuous vessels).
- Requires ongoing imaging follow-up for coil compaction or aneurysm recurrence.
|
💡 Clinical tip: In the UK, coiling is generally first-line for most aneurysms when anatomy permits, especially in older patients or those with comorbidities. Clipping is favoured for younger patients with complex aneurysms or those unsuitable for endovascular access. Decision should be made in a multidisciplinary neurovascular team (MDT) setting.
📈 Prognosis
| Outcome |
Approximate Frequency |
| Death |
30–40% |
| Full recovery |
~30% |
| Permanent disability |
~30% |
📚 References
