💡 Constipation is common, usually benign, but always rule out bowel obstruction first 🚨
(Look for distension, vomiting, absent bowel sounds, hernial orifices, AXR findings).
⚠️ Avoid stimulant laxatives until obstruction excluded.
🌿 Introduction
- Rome IV criteria exist for academic diagnosis [Rome IV link], but most clinical practice is pragmatic.
- Diet: encourage hydration 🥛, mobility 🚶, and fibre (aim 30 g/day). Sorbitol-rich fruits (apples, pears, plums, grapes, raspberries, prunes) are especially helpful.
- Normal variation: stool frequency ranges from twice daily to twice weekly.
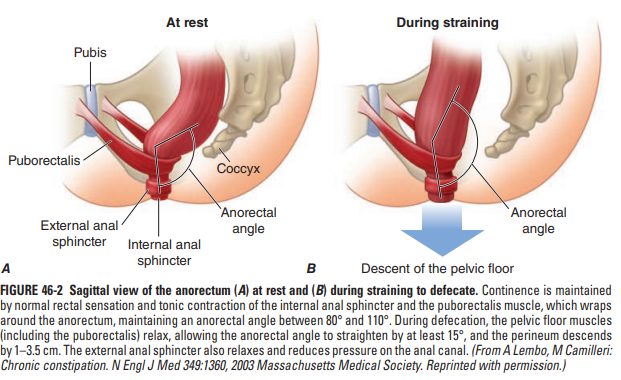
🧠 Anatomy & Physiology of Defaecation
- Colon: absorbs water, compacts stool.
- Rectum: storage; stretch receptors trigger defaecation reflex.
- Anus:
- Internal sphincter: involuntary (smooth muscle)
- External sphincter: voluntary (skeletal muscle)
- Puborectalis muscle: maintains anorectal angle for continence; relaxes during defaecation 💩.
🧾 Common Associations
- Childhood: Hirschsprung’s, cystic fibrosis
- Endocrine/metabolic: hypothyroidism, diabetes, hypercalcaemia, pregnancy
- Neurological: Parkinson’s, MS, spinal cord disease
- Structural: colon cancer, diverticulitis, haemorrhoids
- Medications 💊: opiates, antidepressants, diuretics, CCBs, iron, anticholinergics, NSAIDs, aluminium antacids
- Acute illness: immobility, dehydration
🚩 Red Flags (Investigate)
- PR bleeding, weight loss, family history of colorectal cancer
- Tenesmus, anorexia, night sweats, fever, ↑ inflammatory markers
- Abdominal mass, distension, or pain on PR exam
💊 Laxative Classes
- Bulk-forming: Ispaghula husk (Fybogel) – first-line, needs hydration; avoid in obstruction
- Osmotic: Macrogol (Movicol), Lactulose – for hard stools or opioid-induced constipation; may cause bloating/flatulence
- Stimulant: Senna, Bisacodyl, Sodium Picosulfate – poor propulsion; hydrolysed in colon; avoid if obstruction
- Stool softener: Docusate – adjunct, mild stimulant effect; useful in opioid constipation
- Prokinetic: Prucalopride – severe chronic constipation; 5HT4 agonist; caution in ischaemic heart disease
- Rectal: Phosphate/Microlax/Arachis oil enemas – disimpaction, rapid relief; avoid arachis oil in peanut allergy
🏥 In-Hospital Pearls
- Common triggers: immobility, dehydration, opiates/codeine
- Always examine rectum for hard stool
- Stop causative drugs if possible
- Escalation for disimpaction: Microlax → Phosphate → Arachis oil → Manual removal
💡 Toileting & Lifestyle Advice
- Encourage unhurried, regular routine ⏰
- Respond promptly to urge
- Support mobility and privacy
- Ensure supported seating for frail patients
⚠️ Laxative Cautions
- Avoid in suspected obstruction, perforation, paralytic ileus, toxic megacolon, active IBD flare
- Specific cautions:
- Lactulose: galactosaemia
- Bisacodyl: severe dehydration
- Arachis oil enemas: peanut allergy
- Prolonged overuse → electrolyte imbalance (esp. hypokalaemia)
Cases - Constipation in Adults 🚽
- Case 1 - Functional Constipation 🥖: 45-year-old man, hard stools every 4–5 days, bloating, no red flags. Diet low in fibre.
Management: Lifestyle modification (increase fibre, fluids, exercise); bulk-forming laxatives if required.
- Case 2 - Opioid-Induced Constipation 💊: 62-year-old woman on morphine, painful hard stools.
Management: Regular stimulant + osmotic laxatives; consider peripherally acting opioid antagonist (e.g., naloxegol) if refractory.
- Case 3 - IBS-C 🌿: 35-year-old woman, alternating constipation and bloating, colonoscopy normal.
Management: Dietary advice (low FODMAP), osmotic laxatives (PEG), linaclotide if refractory.
- Case 4 - Secondary Constipation (Hypothyroidism) 🦋: 70-year-old man, lethargy, weight gain, constipation. TFTs: TSH ↑, T4 ↓.
Management: Thyroxine replacement; short-term laxatives if symptomatic.
Teaching Commentary 🧠
Constipation in adults is usually functional, but always consider:
- Primary/functional (diet, IBS, slow transit)
- Secondary (drugs, endocrine, metabolic, neurological)
- Obstructive (colorectal cancer, strictures)
⚠️ Red flags: weight loss, anaemia, rectal bleeding, new onset >50 yrs → urgent colonoscopy
Stepwise management: lifestyle → bulk-forming → osmotic → stimulant → specialist referral if refractory.

