
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Chondrocalcinosis
Related Subjects: |Tennis Elbow |Golfer's Elbow |Painful Shoulder syndromes |Plantar fasciitis |Carpal tunnel syndrome |Chondrocalcinosis |Monoarticular arthritis |Polyarticular arthritis |Seronegative Spondyloarthropathies |Ankylosing spondylitis |Enteropathic Spondyloarthritis |Reactive Arthritis |Psoriatic Arthritis |Adult Onset Still's Disease |Alkaptonuria |Behcet's Syndrome
🦴 About
- Arthritis caused by calcium pyrophosphate deposition (CPPD) in cartilage and periarticular tissues.
- Predominantly affects those over 50 years (younger cases usually suggest an underlying metabolic disorder).
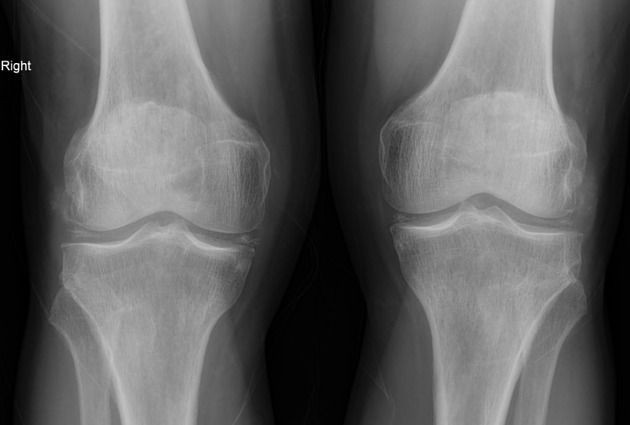
- Most common joint: knee (can also affect wrists, shoulders, hips, and ankles).
- Can mimic gout, rheumatoid arthritis, or osteoarthritis.
- Termed “pseudogout” when it presents with acute monoarthritis.
🧬 Aetiology
- Deposition of calcium pyrophosphate dihydrate crystals within articular cartilage → inflammatory response.
- Chondrocalcinosis on imaging reflects crystal deposition in cartilage.
🩺 Clinical Presentation
- Acute, red, hot, swollen joint – often the knee.
- May present with fever and raised inflammatory markers, mimicking septic arthritis.
- Can cause recurrent acute flares or chronic arthropathy resembling osteoarthritis (esp. in wrists/shoulders).
🔗 Key Associations (classic exam list)
CPPD is frequently linked to metabolic/systemic disease, often tested in MRCP & PACES:
- 🧪 Hyperparathyroidism
- 🩸 Haemochromatosis
- ⚡ Hypomagnesaemia
- 🦋 Hypothyroidism (myxoedematous)
- 🟤 Ochronosis (alkaptonuria)
- 🧬 Wilson's disease
- 💉 Dialysis-dependent renal failure
- 📏 Acromegaly
🔬 Investigations
- Synovial fluid analysis (polarized light microscopy):
- Rhomboid-shaped crystals
- Positively birefringent under polarized light
- 🔎 X-ray: Chondrocalcinosis (linear calcification in cartilage, especially knee meniscus and wrist TFCC).
- Blood tests: screen for metabolic associations (calcium, magnesium, iron studies, thyroid function, renal function).
💊 Management
- 🔹 Acute flare: joint aspiration + intra-articular corticosteroid injection; NSAIDs or colchicine if tolerated.
- 🔹 Supportive: rest, ice, analgesia.
- 🔹 Chronic/recurrent: low-dose colchicine prophylaxis; address underlying metabolic disorder.
- 🔹 Rehabilitation: physiotherapy to maintain joint function and mobility.
Cases - Chondrocalcinosis (Calcium Pyrophosphate Deposition Disease)
- Case 1 - Acute pseudogout flare 💥: A 71-year-old woman presents with acute, painful swelling of her right knee after a minor illness. Joint is hot, red, and tender. Aspirated synovial fluid: positively birefringent, rhomboid-shaped crystals. X-ray: calcification in menisci. Diagnosis: pseudogout attack due to chondrocalcinosis. Treated with NSAIDs and intra-articular steroid injection.
- Case 2 - Chronic arthropathy 🦴: A 66-year-old man with a history of haemochromatosis complains of progressive stiffness and pain in both wrists. Exam: reduced range of motion, no acute synovitis. X-ray: calcification in triangular fibrocartilage and joint space narrowing. Diagnosis: chronic CPPD arthropathy. Managed with analgesia and physiotherapy.
- Case 3 - Secondary cause 🔬: A 58-year-old woman with long-standing hypothyroidism develops recurrent swollen ankles and knees. Synovial fluid shows CPPD crystals. Investigations reveal associated hypomagnesaemia. Diagnosis: secondary chondrocalcinosis. Treated with magnesium replacement and joint-directed therapy.
Teaching Point 🩺: Chondrocalcinosis is due to calcium pyrophosphate deposition in cartilage. It can mimic gout, OA, or RA. Always check for secondary causes (haemochromatosis, hyperparathyroidism, hypomagnesaemia, hypothyroidism). Diagnosis: crystal analysis +
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery