
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Ischaemic Strokes in the Pons
Related Subjects: |Anatomy the Medulla Oblongata |Anatomy of the Midbrain |Anatomy of the Pons
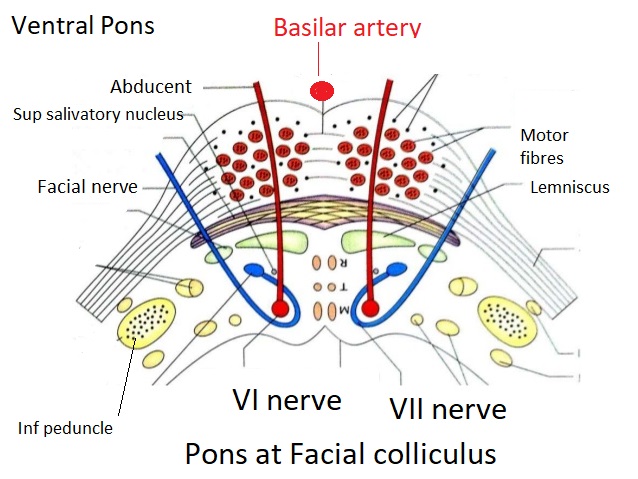
🧠 Note: Anatomical diagrams of the pons are often displayed inverted compared to radiological (CT/MRI) orientation - except as shown below. This distinction is important when correlating anatomy with clinical findings or interpreting imaging.
🌉 Introduction
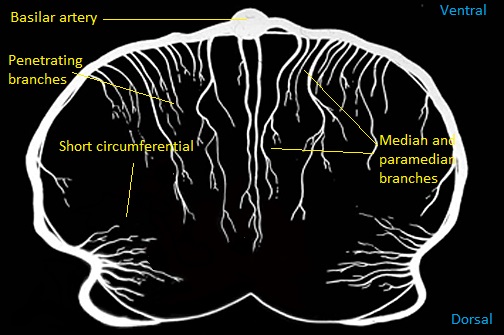
- 🩸 Pontine strokes are most often lacunar infarcts due to occlusion of small penetrating arteries from the basilar trunk.
- 📈 Common risk factors include age, hypertension, diabetes, and atherosclerosis.
- ⚠️ Bilateral lesions are uncommon but can occur with basilar artery occlusion - potentially devastating with “locked-in” presentation.
🧬 Aetiology
- 🎯 Usually small-vessel occlusion of penetrating branches of the basilar artery → unilateral pontine infarcts.
- 🫀 Basilar occlusion at the origins of perforators → possible bilateral pontine infarction.
- 🔄 Shared risk factors with other small-vessel strokes: hypertension, diabetes, ageing, and lipohyalinosis.
- 🚫 Large-vessel infarcts (basilar atherothrombosis, embolism) → wider territory infarction ± coma.
- 💧 Oedema near 4th ventricle may obstruct CSF flow → acute hydrocephalus requiring ventricular drainage.
🧩 Clinical Features
- ⚡ Contralateral hemiparesis or hemisensory loss - corticospinal and medial lemniscus involvement.
- 🚫 No cortical signs (e.g., aphasia, neglect, hemianopia) - helps differentiate from cortical stroke.
- 🙂 Ipsilateral facial palsy (LMN type) - facial nucleus or fascicle lesion.
- 👀 Diplopia or lateral gaze palsy - due to abducens (VI) nerve involvement.
- 🔒 Locked-in syndrome: Quadriplegia + anarthria but preserved consciousness and vertical eye movement.
- 🌀 Vertigo, nystagmus, ataxia - if cerebellar peduncles affected.
- 🔥 Pyrexia & autonomic instability - involvement of reticular or hypothalamic pathways.
- 🗣️ Dysarthria–clumsy hand syndrome or pure motor stroke presentations (lacunar syndromes).
- 🔁 Fluctuating symptoms - “pontine warning syndrome”, similar to capsular warning episodes.
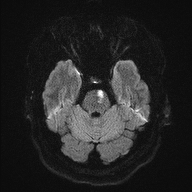
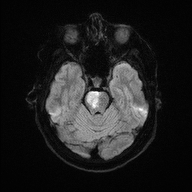
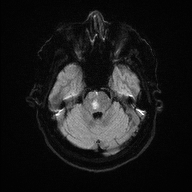
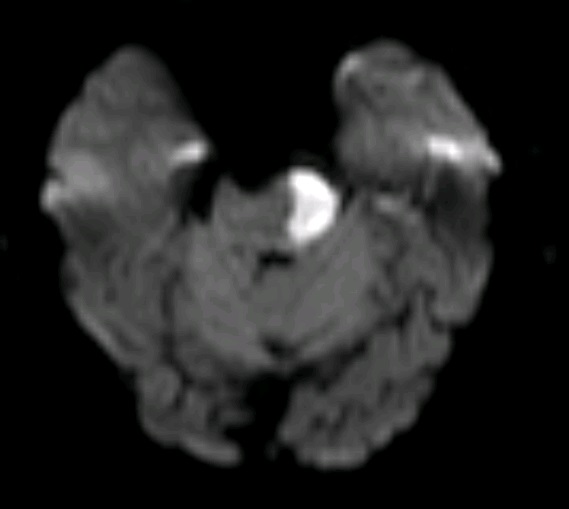
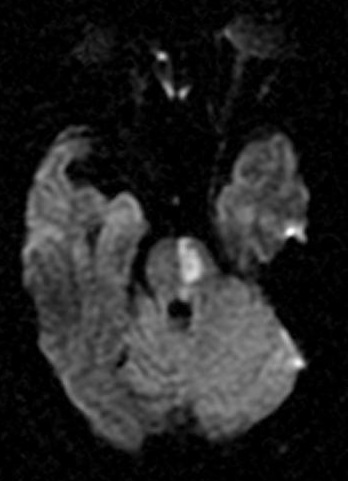
🖼️ Anatomical & Imaging Examples
📍 Pontine infarcts typically respect the midline and may extend posteriorly toward the cerebellum.

🧪 Investigations
- 🩸 Routine bloods: FBC, U&E, LFTs, glucose, lipid profile.
- 🧠 CT ± CTA: To confirm acute stroke, rule out haemorrhage, and assess basilar patency.
- 🧲 MRI brain: More sensitive for small infarcts - DWI highlights acute ischaemia early.
- 🔍 MRA / CTA: Evaluate for vertebrobasilar stenosis or occlusion.
🩺 Management
- 💉 Reperfusion therapy: IV thrombolysis (within window) or thrombectomy for basilar occlusion - improves survival in selected patients.
- 🏥 Stroke Unit care: Multidisciplinary monitoring, oxygenation, and early rehab initiation.
- 💊 Antiplatelet: Aspirin 300 mg ± Clopidogrel after imaging confirms ischaemia.
- ⚖️ Risk factor control: Optimize BP, glucose, and address AF or dyslipidaemia.
- 🧠 Statins: Start high-intensity statin (e.g., atorvastatin 80 mg) for secondary prevention.
- 🗣️ Rehabilitation: Physiotherapy, occupational therapy, and speech therapy for motor/speech recovery and swallow safety.
💡 Teaching tip: Pontine strokes are often clinically silent or subtle initially but may deteriorate rapidly. Always assess eye movements, facial symmetry, and bulbar function in any suspected brainstem event. Locked-in syndrome is the hallmark of extensive bilateral pontine infarction - preserved awareness but paralysis below the eyes.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery