Related Subjects:
|Antepartum haemorrhage
|Postpartum haemorrhage
|Acute Haemorrhage
|Placenta praevia
|Placenta abruption
|Anti-D immunoglobulin
⚠️ About
- Placenta praevia = placenta implanted in lower uterine segment, covering/reaching internal cervical os.
- Major cause of painless antepartum haemorrhage in 2nd–3rd trimester → usually requires Caesarean delivery.
- 🚨 Avoid digital vaginal examination if suspected → can trigger catastrophic bleeding.
📊 Aetiology
- Incidence ~1 in 200 pregnancies.
- Bleeding can be severe/rapid due to uterine blood flow (600–800 mL/min at term).
- USS in early pregnancy may show “low-lying placenta” → usually migrates upward with uterine growth, but persistent low position = praevia.
⚠️ Risk Factors
- Previous Caesarean section (scar tissue, abnormal placental implantation)
- Multiparity & multiple pregnancy → larger placental surface area
- Uterine abnormalities (fibroids, prior uterine surgery)
- Smoking, advanced maternal age
🩺 Clinical Features
- Painless vaginal bleeding (classically at 29–30 wks or later).
- Uterus soft, non-tender (contrast with abruption).
- Fetal heart rate usually normal (unless severe haemorrhage).
- Speculum exam may show blood, but digital VE contraindicated.
- Often abnormal lie/presentation (e.g. transverse/oblique) due to placental obstruction of lower segment.
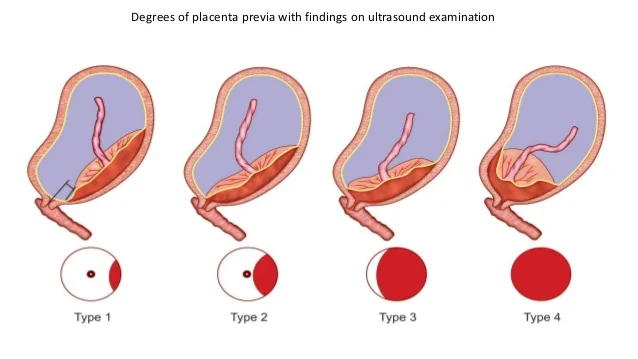
📑 Grades of Placenta Praevia
- Complete: placenta fully covers os
- Partial: placenta partially covers os
- Marginal: placenta reaches os edge but does not cover
- Low-lying: in lower segment but does not reach os
🔍 Differential Diagnosis
- Placental abruption: painful, tender uterus, often concealed bleeding
- Local genital causes: cervical polyp, infection, trauma
🧪 Investigations
- Transvaginal USS: gold standard (safer & more accurate than transabdominal).
- Bloods: FBC, group & cross-match, clotting screen, U&E.
- CTG: fetal monitoring.
🏥 Management
- Stabilise mother first: IV access, fluids, cross-match, transfuse as needed (Hb >10 g/dL).
- Hospital admission: if recurrent bleeding or major praevia; sometimes recommended from 35 weeks.
- Steroids: if <34 wks → promote fetal lung maturity.
- Definitive delivery: planned Caesarean section at 37–38 wks, earlier if bleeding or distress. Consultant-led care essential.
⚠️ Complications
- Maternal haemorrhage & shock
- Preterm labour or iatrogenic preterm delivery
- Placenta accreta spectrum (invasion into myometrium) → risk of massive PPH
- Malpresentation (breech, transverse)
📌 Exam Pearls
- Placenta praevia = painless bleeding, soft uterus, normal FHR
- Placental abruption = painful, tense uterus, fetal distress
- Always confirm with USS before VE
- Low-lying placenta at 20 wks often resolves; persistence into 3rd trimester = praevia
