| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Caroticocavernous Fistula
🚨 Red Flag: Acute unilateral pulsatile tinnitus with objective orbital bruit = suspect high-flow CCF (Type A) until proven otherwise. Vision loss risk and rare SAH risk mandate urgent neurovascular referral.
🩺 Introduction & Relevant Anatomy
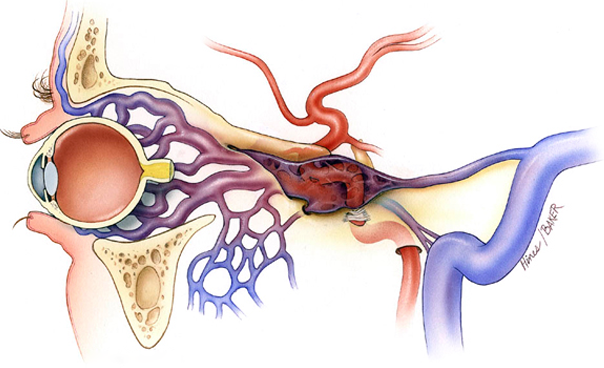
- Abnormal arteriovenous shunt between carotid arterial system and cavernous sinus.
- Cavernous sinus contains: ICA, CN III, IV, V1, V2 (lateral wall), and VI (within sinus).
- Arterialisation of venous sinus → retrograde flow into superior ophthalmic vein → orbital venous congestion.
- Leads to raised episcleral venous pressure → ↑ intraocular pressure and secondary glaucoma.
🧬 Aetiology
- Direct (High-flow, Barrow A):
- Blunt or penetrating head trauma (most common)
- Ruptured cavernous ICA aneurysm
- Connective tissue disorders (e.g. vascular Ehlers-Danlos)
- Indirect (Low-flow, Barrow B–D):
- Dural AV fistula from meningeal branches of ICA and/or ECA
- More common in postmenopausal women
- Associated with hypertension or spontaneous development
📊 Clinical Features
- Classic triad: Pulsatile tinnitus, proptosis, chemosis.
- Objective bruit over orbit/temple (pathognomonic clue).
- Dilated “arterialised” episcleral veins.
- Raised IOP → secondary glaucoma.
- Diplopia from CN III, IV, VI palsy (VI most vulnerable).
- Reduced visual acuity if optic nerve congestion.
🚨 Red Flags (Urgent Intervention)
- Progressive vision loss.
- Severe proptosis with exposure keratopathy.
- Acute high-flow bruit.
- Cranial neuropathies.
- Signs of SAH (rare but serious).
🔎 Investigations
- CTA: First-line for suspected direct CCF; enlarged cavernous sinus, dilated superior ophthalmic vein.
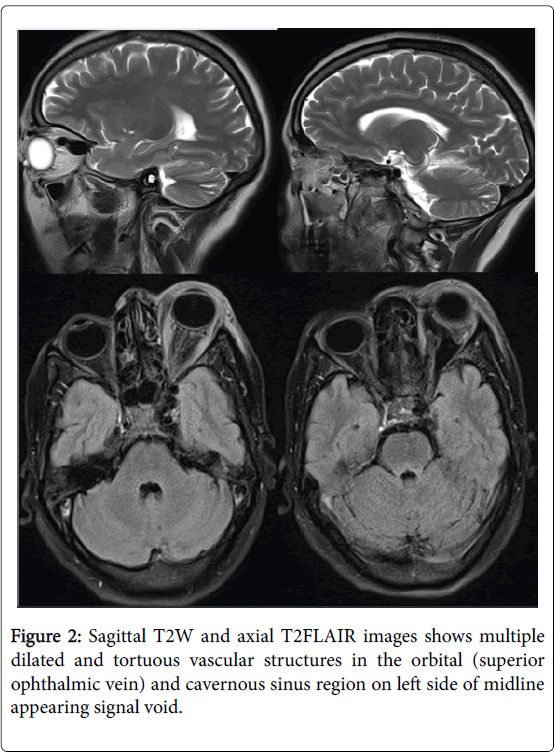
- MRI/MRV: Better for indirect fistulas; flow voids, venous congestion.
- DSA: Gold standard. Defines arterial feeders, venous drainage pattern, and treatment route.
- Ophthalmic assessment: IOP, fundoscopy (venous stasis retinopathy).
📚 Barrow Classification (1985)
| Type | Description | Flow | Typical Cause |
|---|---|---|---|
| A | Direct ICA → cavernous sinus | High-flow | Trauma / aneurysm rupture |
| B | ICA meningeal branches → cavernous sinus | Low-flow | Spontaneous dural AVF |
| C | ECA meningeal branches → cavernous sinus | Low-flow | Spontaneous dural AVF |
| D | ICA + ECA meningeal branches → cavernous sinus | Low-flow | Most common indirect type |
🔍 Differentials
- Graves’ orbitopathy (bilateral, no bruit).
- Cavernous sinus thrombosis (septic features, bilateral).
- Orbital cellulitis.
- Superior ophthalmic vein thrombosis.
- Idiopathic intracranial hypertension (pulsatile tinnitus but no chemosis/proptosis).
💊 Management
- Urgent specialist referral (neurosurgery/interventional neuroradiology).
- High-flow Type A: Endovascular embolisation first-line (transarterial approach; coils, liquid embolics). Success 90–95%.
- Low-flow Types B–D: Often conservative initially; spontaneous closure possible.
- Intervene if visual deterioration, intolerable bruit, glaucoma, or progressive symptoms.
- Supportive: IOP-lowering drops, acetazolamide, corneal protection.
🧠 Clinical Exam Pearl
Unilateral red eye + pulsatile tinnitus + bruit = think CCF. VI nerve palsy is the most common cranial nerve deficit due to its intraluminal position within the cavernous sinus.
📖 Evidence & References
- StatPearls: Carotid Cavernous Fistula (updated 2024–2025)
- Radiopaedia: CCF & Barrow Classification
- JNIS / Frontiers Neurology (2024–2025 endovascular outcome series)
- AAO EyeWiki (2025 update)