⚠️ Acute liver disease is not the same as acute liver failure.
Acute liver disease may range from mild hepatocellular injury to life-threatening acute liver failure (ALF).
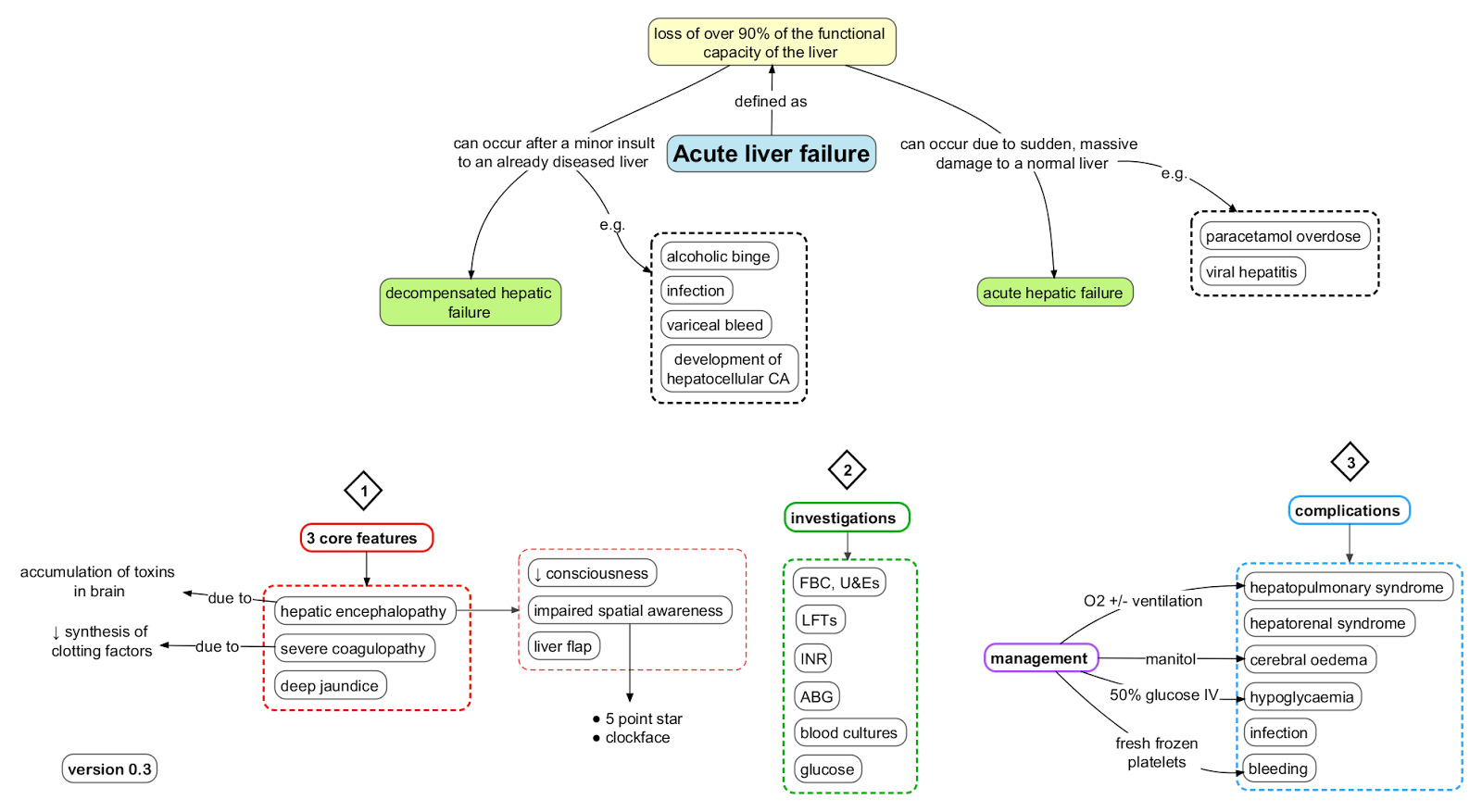
ALF is defined by acute liver injury with impaired synthetic function, usually INR ≥1.5, plus hepatic encephalopathy, in a patient without known pre-existing cirrhosis.
🩺 Acute Liver Disease & Acute Liver Failure
- Acute liver injury: sudden hepatocellular injury with raised ALT/AST, but without encephalopathy.
- Acute severe hepatitis: severe liver injury with jaundice and coagulopathy, but no encephalopathy yet.
- Acute liver failure: acute liver injury with coagulopathy and hepatic encephalopathy.
- Acute-on-chronic liver failure: acute deterioration in a patient with known or previously unrecognised chronic liver disease.
- 🚨 ALF is a medical emergency because deterioration can be rapid, with cerebral oedema, hypoglycaemia, sepsis, renal failure and multiorgan failure.
📊 Classification of Acute Liver Failure
| Type |
Jaundice → Encephalopathy |
Common Causes |
Key Features |
| Hyperacute |
<7 days |
💊 Paracetamol toxicity, HAV, HBV, HEV, ischaemic hepatitis |
Rapid deterioration, high cerebral oedema risk, but potentially better transplant-free survival if treated early. |
| Acute |
8–28 days |
🦠 Viral hepatitis, drug-induced liver injury, autoimmune hepatitis |
Cerebral oedema possible; prognosis depends strongly on cause and severity. |
| Subacute |
5–12 weeks |
💊 Drug-induced injury, autoimmune, viral, indeterminate, Wilson disease |
Less cerebral oedema than hyperacute ALF, but often worse spontaneous recovery. |
🧠 Causes of Acute Liver Disease & ALF
- 💊 Paracetamol toxicity: most important treatable cause in the UK; risk increased by delayed presentation, staggered overdose, alcohol misuse or malnutrition.
- 💊 Other drugs/toxins: antibiotics, antiepileptics, NSAIDs, statins, antituberculous therapy, herbal remedies, recreational drugs, Amanita phalloides mushrooms.
- 🦠 Viral hepatitis: HAV, HBV, HEV; also HSV, VZV, EBV, CMV and adenovirus, especially in pregnancy or immunosuppression.
- 🛡 Autoimmune hepatitis: may present acutely or as ALF.
- 🧬 Metabolic: Wilson disease, acute fatty liver of pregnancy, Reye syndrome.
- 🤰 Pregnancy-related: HELLP syndrome, acute fatty liver of pregnancy, severe pre-eclampsia.
- 🩸 Vascular/ischaemic: shock liver, Budd–Chiari syndrome, heatstroke, severe cardiac failure.
- 🍷 Alcoholic hepatitis: causes acute severe liver disease but often occurs on a background of chronic liver injury, so distinguish from true ALF.
- ❓ Indeterminate: no cause found despite investigation.
🩺 Clinical Features
- 🤢 Nausea, vomiting, anorexia, malaise and abdominal pain.
- 🟡 Jaundice, dark urine, pale stools and pruritus.
- 🧠 Encephalopathy: sleep disturbance, confusion, agitation, asterixis, reduced consciousness or coma.
- 🩸 Bleeding or bruising from coagulopathy.
- 🍬 Hypoglycaemia, especially in severe hepatocellular failure.
- 🫀 Right upper quadrant pain or tender hepatomegaly may occur.
- 🚫 Stigmata of chronic liver disease are usually absent in true ALF.
🧠 Hepatic Encephalopathy Grades
| Grade |
Clinical Features |
| Grade 1 |
Sleep disturbance, poor concentration, mild confusion, irritability or altered behaviour. |
| Grade 2 |
Drowsiness, disorientation, asterixis, personality change. |
| Grade 3 |
Marked confusion, somnolence, incoherent speech, responds to pain/voice. |
| Grade 4 |
Coma, may be unresponsive to pain. |
🩺 Acute Liver Failure vs Chronic Liver Disease
| Feature |
Acute Liver Failure ⚡ |
Chronic Liver Disease 🕰️ |
| Onset ⏱️ |
Rapid: days to weeks. |
Gradual: months to years. |
| Encephalopathy 🧠 |
Early and rapidly progressive. |
Usually later or precipitated by infection, GI bleed, constipation, sedatives or renal failure. |
| Coagulopathy 🩸 |
INR rises early due to acute loss of synthetic function. |
May be chronically abnormal; synthetic failure often evolves over time. |
| Ascites 💧 |
Usually absent at first, may develop later. |
Common with portal hypertension. |
| Splenomegaly 🌳 |
Usually absent. |
Common due to portal hypertension. |
| Spider naevi / palmar erythema 🕷️ |
Usually absent. |
Common stigmata of chronic liver disease. |
| Muscle wasting 💪 |
Usually absent initially. |
Common in advanced chronic liver disease. |
💡 Clinical tip: AST/ALT tell you about hepatocyte injury; INR, glucose, lactate, bilirubin trend and encephalopathy tell you about liver failure.
A patient can have ALT >1000 without liver failure, but confusion plus INR elevation is an emergency.
🔎 Initial Investigations
| Investigation |
Why It Matters |
| LFTs: ALT, AST, ALP, GGT, bilirubin |
Pattern of injury: hepatocellular, cholestatic or mixed. |
| INR / PT |
Key marker of synthetic failure and prognosis. |
| Glucose |
Hypoglycaemia is common in severe ALF and can be fatal. |
| U&E, creatinine, phosphate, magnesium |
Renal failure and electrolyte abnormalities are common. |
| FBC, CRP, cultures |
Assess infection, sepsis, anaemia and platelet count. |
| ABG/VBG, lactate, pH |
Acidosis and lactate are important severity markers, especially in paracetamol toxicity. |
| Paracetamol level |
Check in all unexplained acute hepatitis or ALF, even if overdose is denied. |
| Toxicology screen |
Consider drugs, toxins, recreational substances and poisoning. |
| Viral screen |
HAV IgM, HBsAg, anti-HBc IgM, HBV DNA, HCV Ab/RNA, HEV IgM/RNA; consider HSV/VZV/EBV/CMV. |
| Autoimmune screen |
ANA, SMA, LKM antibodies, IgG. |
| Metabolic tests |
Caeruloplasmin, copper studies, ferritin, transferrin saturation, alpha-1 antitrypsin if indicated. |
| Pregnancy test |
Essential in women of childbearing potential; consider HELLP and acute fatty liver of pregnancy. |
| Ultrasound liver + Doppler |
Assess biliary obstruction, hepatic/portal vein thrombosis, Budd–Chiari, tumour and chronic liver morphology. |
🚑 Immediate Management
- 🚨 Escalate early: involve senior medical, ICU, hepatology and a liver transplant centre if ALF is suspected.
- 🔄 ABCDE assessment: protect airway, give oxygen if needed, support circulation and monitor mental state.
- 🛌 Admit to HDU/ICU if encephalopathy, rising INR, hypoglycaemia, acidosis, renal failure, severe vomiting, sepsis or rapid deterioration.
- 🍬 Prevent hypoglycaemia: frequent glucose checks and IV dextrose if needed.
- 💧 Fluids and electrolytes: correct hypovolaemia, sodium, potassium, phosphate and magnesium carefully.
- 🦠 Infection: culture and treat suspected sepsis promptly; avoid unnecessary delays.
- 🧠 Encephalopathy: avoid sedatives where possible; manage airway risk; treat cerebral oedema urgently if suspected.
- 🩸 Coagulopathy: do not correct INR routinely with FFP unless bleeding or before invasive procedures, because INR is a key prognostic marker.
- 🧪 Serial monitoring: INR, LFTs, glucose, lactate, pH, renal function, phosphate and conscious level.
- 🚫 Avoid hepatotoxins: alcohol, unnecessary paracetamol, NSAIDs and sedatives.
💊 Cause-Specific Treatment
- 💊 Paracetamol toxicity: give IV N-acetylcysteine immediately if indicated; do not wait if high suspicion or delayed presentation.
- 💊 Non-paracetamol ALF: N-acetylcysteine may still be considered early under specialist guidance.
- 🦠 HSV/VZV hepatitis: IV aciclovir if suspected, especially in pregnancy or immunosuppression.
- 🦠 Severe acute HBV: discuss nucleos(t)ide analogue therapy such as tenofovir or entecavir with hepatology.
- 🛡 Autoimmune hepatitis: corticosteroids may be considered by specialists after infection and sepsis are assessed.
- 🍄 Amanita mushroom poisoning: urgent toxicology/hepatology input; consider silibinin where available and transplant assessment.
- 🤰 Pregnancy-related disease: urgent obstetric, anaesthetic and hepatology input; delivery is definitive treatment for HELLP/acute fatty liver of pregnancy.
- 🧬 Wilson disease ALF: urgent transplant-centre discussion; prognosis without transplant is poor.
- 🩸 Budd–Chiari syndrome: anticoagulation and specialist consideration of thrombolysis, TIPS or transplant.
- 🫀 Ischaemic hepatitis: treat shock, hypoxia or cardiac failure.
👑 King’s College Criteria - Transplant Assessment
🚑 King’s College criteria help identify patients who may need urgent liver transplantation.
They do not replace clinical judgement: discuss early with a liver transplant centre if ALF is suspected, especially with encephalopathy, rising INR, acidosis, renal failure or lactate elevation.
| Cause |
Criteria Suggesting Poor Prognosis / Transplant Need |
| Paracetamol-related ALF |
Arterial pH <7.3 after fluid resuscitation
OR
All 3 of: INR >6.5, creatinine >300 micromol/L, and grade 3–4 encephalopathy.
|
| Non-paracetamol ALF |
INR >6.5 regardless of encephalopathy grade
OR
Any 3 of: age <10 or >40 years, non-A/non-B hepatitis or drug-induced cause, jaundice-to-encephalopathy interval >7 days, INR >3.5, bilirubin >300 micromol/L.
|
🧠 Cerebral Oedema & Raised ICP
- More common in hyperacute ALF and grade 3–4 encephalopathy.
- Warning signs: falling GCS, agitation, pupillary changes, hypertension/bradycardia, seizures or abnormal posturing.
- Manage in ICU with head-up positioning, avoidance of hypoxia/hypotension, controlled ventilation if intubated, and specialist osmotherapy such as hypertonic saline or mannitol.
- Avoid hyponatraemia and fever; maintain adequate cerebral perfusion.
⚠️ Complications
- 🍬 Hypoglycaemia.
- 🩸 Coagulopathy and bleeding.
- 🧠 Cerebral oedema and raised intracranial pressure.
- 🦠 Infection and sepsis.
- 🫘 Acute kidney injury and hepatorenal physiology.
- 🫁 Respiratory failure or aspiration.
- 🧪 Metabolic acidosis, lactate elevation and electrolyte abnormalities.
- 🫀 Multiorgan failure.
📝 Exam Pearls
- ⚠️ Acute liver injury becomes acute liver failure when there is coagulopathy plus encephalopathy.
- 🧪 ALT >1000 suggests paracetamol toxicity, viral hepatitis or ischaemic hepatitis.
- 🩸 INR is more important than ALT for assessing liver failure severity.
- 🍬 Always check glucose: hypoglycaemia can be life-threatening.
- 💊 Check a paracetamol level even if overdose is not disclosed.
- 🚑 Early transplant-centre discussion saves lives; do not wait until the patient is moribund.
- 🧠 Lactulose is standard for chronic hepatic encephalopathy, but in ALF the priority is ICU-level cerebral oedema and airway management.
🧠 Teaching Note
Acute liver failure is dangerous because the liver suddenly loses its ability to perform synthetic, metabolic and detoxifying functions.
INR rises because clotting factors have short half-lives, glucose falls because hepatic glycogen and gluconeogenesis fail, and encephalopathy develops as toxins and inflammatory mediators affect the brain.
Marked ALT/AST means hepatocytes are injured, but it does not by itself prove liver failure.
The key bedside question is: is the patient coagulopathic, hypoglycaemic, acidotic or encephalopathic?
📚 References & UK Resources

