Related Subjects:
|Neurological History taking
|Alzheimer disease
|Dementia with Lewy bodies
|Frontotemporal dementia
|Corticobasal degeneration
|Creutzfeldt Jakob disease
|Vascular Dementia
|Ischaemic Stroke
|Hypertension
|CADASIL
|CARASIL
| 🚫 Reasons why MRI may not be possible |
|---|
- 📉 MRI scanner unavailable, Swan-Ganz catheter in situ
- 🧲 Brain aneurysm clips (check with manufacturer), deep brain stimulator
- 👁️ Ocular metallic foreign bodies (skull X-ray can help exclude)
- 🏥 Patient too ill to monitor safely in MRI environment
- 😰 Extreme claustrophobia
- ❤️ Pacemaker/AICD, recent surgery with clips or metallic implants
- 💉 Insulin pumps, neurostimulators, cochlear implants may be de-programmed
- 🛌 Unable to lie flat (MSK or cardiorespiratory reasons, kyphosis, obesity)
- 🔫 Bullets or gunshot pellets near vital organs (lungs, heart, brain)
- 🤰 Early pregnancy (relative C/I - limited data)
- 🧠 Cognitive impairment or agitation (sometimes sedation required)
|
🧲 MRI Basics
- ⚡ Unlike CT, which uses ionising radiation, MRI uses radio waves + magnetic fields. ✅ No radiation risk.
- 📸 MRI provides high-resolution, multiplanar imaging (axial, sagittal, coronal, oblique).
- 🔬 CT pixel intensity = electron density; MRI = hydrogen (H⁺ nuclei) density modified by tissue relaxation times (T1, T2).
- 🌀 Hydrogen protons align in strong magnetic field; gradients encode spatial location.
- 🛠️ MRI components: main magnet, gradient coils, RF transmitter/receiver, computer for image reconstruction.
- 📡 Emitted “spin echo” at the Larmor frequency → Fourier transform → detailed image.
💡 Teaching pearl: MRI signal depends not only on hydrogen density but also on tissue environment (T1, T2 relaxation, flow, diffusion).
⚠️ Challenges of MRI Scanning
- ⏱️ Scan duration: 10–30 min → difficult for claustrophobic/anxious patients.
- 🔊 MRI is noisy; limited communication during scan.
- 🏥 Open MRI exists for claustrophobia, but limited availability.
- 🎯 Aim: shortest protocol to answer the clinical question.
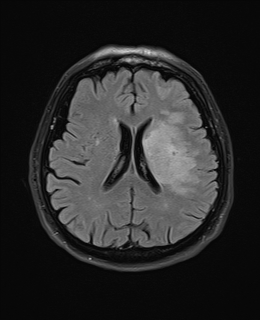
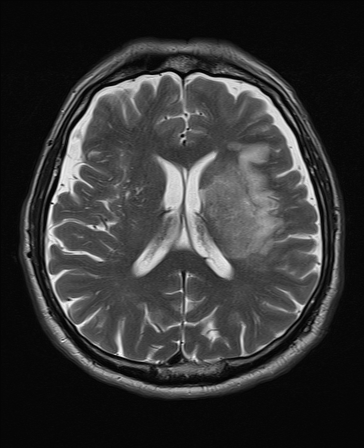
📸 Examples
| T2 FLAIR | T2 |
|---|
 |  |
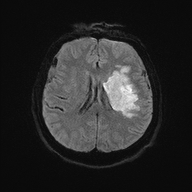
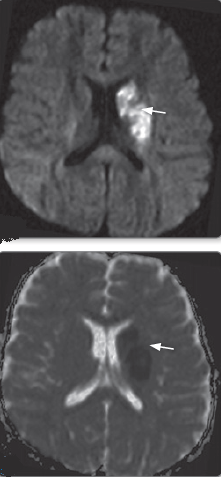
| DWI | ADC |
|---|
 |  |
| SWI | T1 Sagittal |
|---|
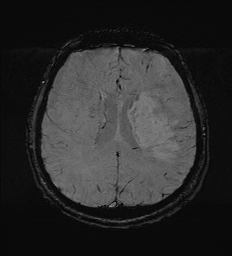 | 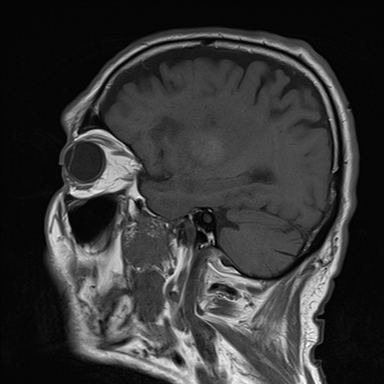 |
🛡️ MRI Safety Considerations
- Most prosthetic valves, IVC filters, vascular stents, IUDs, and metallic prostheses are MRI-safe ✅.
- Key risk = movement or heating of ferromagnetic implants. Always check manufacturer guidance.
- Resources: MRI Contraindications Policy
| MRI Safety.com
💉 MRI with Gadolinium
- Contrast shortens T1 → brighter images. Used for tumours, inflammation, abscess, meningitis.
- Not usually needed in acute stroke unless diagnostic uncertainty.
📊 Understanding MRI Sequences
- ⏳ T1: Fat bright, CSF dark. Best for anatomy. Acute stroke = hypointense.
- 💧 T2: Water bright, fat darker. Best for oedema/infarcts.
- ⭐ T2* / GRE: Detects blood products, iron, microbleeds.
- 🚫 FLAIR: Suppresses CSF signal → highlights periventricular oedema/lesions.
- ⚡ DWI/ADC: Bright in acute ischaemic stroke (cytotoxic oedema).
- 🧲 SWI: Very sensitive to blood/iron → detects microbleeds & calcification.
🧠 Imaging Patterns in Stroke
| Condition | Imaging Characteristics |
|---|
| 🚑 Acute Ischaemic Stroke | DWI bright (acute), ADC low; FLAIR/T2 hyperintense after few hours; GRE may show thrombosis. |
| ❤️ Cardioembolic Stroke | Multiple vascular territories, varying lesion ages. |
| 🎯 Lacunar Stroke | Small, round lesions (<1.5 cm) in deep brain regions (thalamus, pons, internal capsule). |
| 🧵 Carotid Dissection | Fat-suppressed T2 shows thrombus; CTA/MRA for obstruction. |
| 🔒 Basilar Artery Occlusion | Hyperdense basilar sign (CT), confirmed on CTA/MRA. |
🩸 Imaging Patterns in Haemorrhage
| 💥 Hypertensive Haemorrhage | Common in putamen, thalamus, pons. GRE/T2* sensitive to microbleeds. |
| 🧓 Cerebral Amyloid Angiopathy | Microbleeds in temporal/occipital lobes; GRE/T2* detects 2 mm bleeds. |
📖 Exam pearls:
- DWI = most sensitive for acute stroke (<30 mins).
- GRE/T2* = microbleeds and haemorrhage detection.
- FLAIR = MS plaques, periventricular oedema.
- T1 = anatomy & post-contrast detail.
