⚠️ Cerebral vasculitis is frequently overdiagnosed due to over-interpretation of angiographic “beading”.
Catheter angiography is neither sensitive nor specific.
Immunosuppressive treatments are toxic - establish diagnosis carefully before treatment.
🩺 Introduction
- Inflammation of cerebral blood vessels leading to stenosis, occlusion, thrombosis, or haemorrhage.
- May be primary (PACNS) or secondary to systemic vasculitis, infection, malignancy, or autoimmune disease.
- No single clinical, blood, or imaging test is diagnostic.
- Diagnosis is clinicoradiological and often requires biopsy.
🧬 Aetiology
- Immune-mediated endothelial injury.
- Immune complex deposition in vessel walls.
- ANCA-associated mechanisms.
- Genetic and environmental triggers.
- Secondary causes: infection (TB, HIV, syphilis), malignancy, drugs, connective tissue disease.
📊 Size-Based Classification (Systemic Context)
| Vessel Size |
Examples |
| Large Vessel |
Giant Cell Arteritis, Takayasu arteritis |
| Medium Vessel |
Polyarteritis nodosa, Kawasaki disease |
| Small Vessel |
- ANCA-positive: Granulomatosis with polyangiitis (GPA), Microscopic polyangiitis (MPA), Eosinophilic granulomatosis with polyangiitis (EGPA)
- ANCA-negative: Cryoglobulinaemic vasculitis, Behçet disease
- Primary Angiitis of the CNS (PACNS)
|
🧠 Primary Angiitis of the CNS (PACNS)
- Inflammatory vasculitis confined to CNS.
- Any age; typically subacute headache, cognitive decline, focal deficits.
- CSF abnormal in ~80% (raised protein, lymphocytosis).
- Angiography may show segmental narrowing (“beading”) but not diagnostic.
- Brain/leptomeningeal biopsy is gold standard (may be false negative in segmental disease).
🔎 Clinical Features
- Headache (commonest symptom).
- Ischaemic stroke (single or multiple territories).
- Intracerebral haemorrhage.
- Seizures.
- Encephalopathy.
- Systemic features if secondary vasculitis (rash, renal impairment, arthritis).
🔬 Investigations
- Bloods: ESR, CRP, FBC, U&E, LFTs.
- Autoimmune screen: ANA, dsDNA, ANCA (PR3/MPO), complement, RF.
- Infection screen: HIV, Hep B/C, syphilis, TB.
- Urinalysis for glomerulonephritis.
- CSF: Raised protein ± lymphocytes (PACNS often inflammatory).
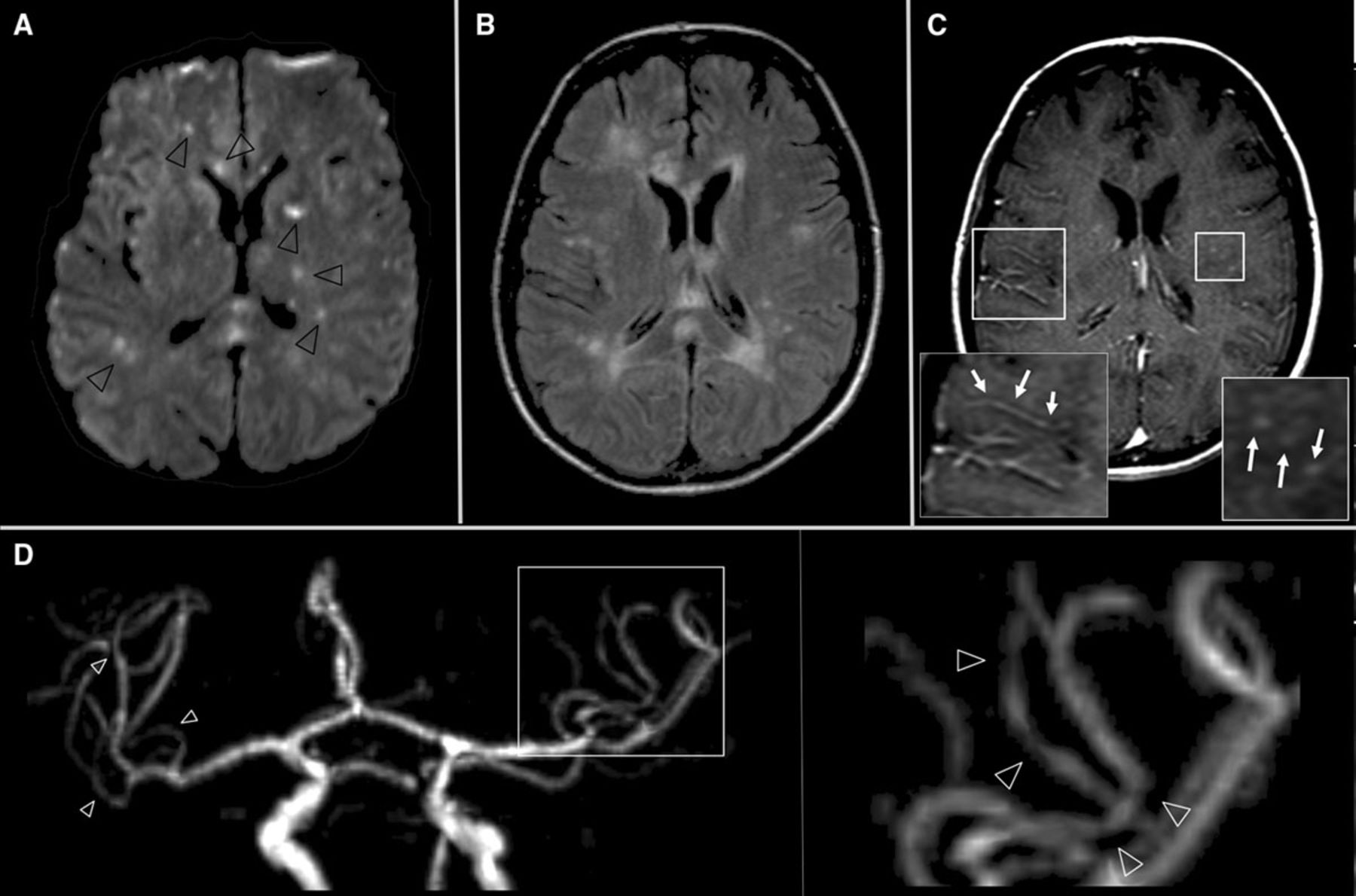
- MRI brain: Multifocal infarcts of different ages; haemorrhage; vessel wall enhancement on high-resolution imaging.
- DSA: May show segmental stenosis and dilatation (“string-of-beads”).
- FDG-PET: Helpful in large vessel systemic vasculitis.
- Biopsy: Definitive diagnosis if positive.
⚖️ Differential Diagnosis of Angiographic “Beading”
- Reversible Cerebral Vasoconstriction Syndrome (RCVS).
- Fibromuscular dysplasia.
- Vasospasm (post-SAH).
- Atherosclerosis.
- Infection-related vasculopathy.
- Embolic phenomena.
💊 Management Principles
- Confirm diagnosis before immunosuppression where possible.
- Exclude infection (critical before steroids).
- Induction therapy: High-dose corticosteroids ± cyclophosphamide.
- Alternative induction: Rituximab (especially ANCA-associated).
- Maintenance: Azathioprine, methotrexate, or mycophenolate mofetil.
- Monitor for drug toxicity (cytopenias, infection, bladder toxicity with cyclophosphamide).
🧠 Clinical Pearl
Not all angiographic beading is vasculitis.
RCVS is far more common and does not require immunosuppression.
Treating presumed vasculitis without adequate evidence can cause significant harm.
📚 Reference
- Berlit P. Diagnosis and treatment of cerebral vasculitis. Ther Adv Neurol Disord (2010).
