
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Bladder
Related Subjects: |Anatomy of the Glomerulus |Anatomy of the Bladder
🫙 The urinary bladder is a hollow, distensible muscular sac in the pelvis that temporarily stores urine (typically 400–600 mL comfortably, up to 800–1000 mL max) before voluntary voiding. It expands dramatically during filling (compliance ~20–40 mL/cm H₂O) and contracts forcefully during micturition to expel urine via the urethra.
🧬 Anatomy of the Bladder
- Location & Relations 📍
- Lies in the true pelvis, behind the pubic symphysis, anterior to the rectum (males) or uterus/vagina (females).
- Superior surface covered by peritoneum → forms anterior peritoneal reflection (vesicouterine/vesicorectal pouch).
- Males: prostate inferiorly, seminal vesicles posteriorly.
- Females: uterus/vagina posteriorly, pubic symphysis anteriorly.
- When full: rises above pubic symphysis → palpable/percussible in lower abdomen.
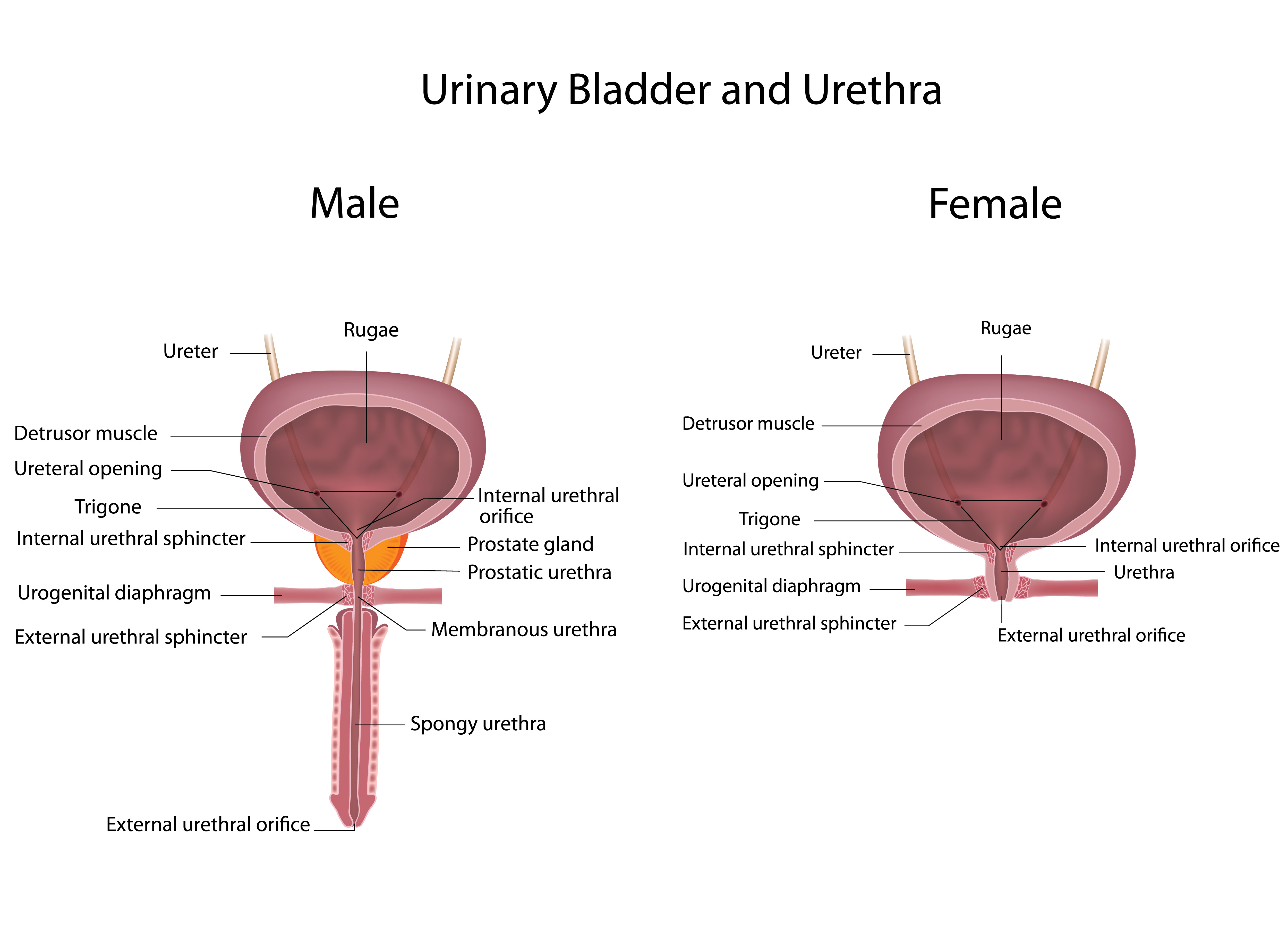
- External Features
- Apex (Fundus anterior): Superior/anterior point; attached to median umbilical ligament (urachus remnant).
- Base (Fundus posterior): Triangular posterior wall; ureters enter superolaterally.
- Body: Main expandable portion between apex and base.
- Neck: Inferior constriction; continuous with prostatic urethra (males) or urethra (females).
- Internal Features – Trigone 🔺
- Smooth, fixed triangular area on posterior base.
- Boundaries: two ureteric orifices (superolateral) + internal urethral orifice (inferior apex).
- Lined by tightly adherent mucosa (no rugae) → less distensible; embryologically mesodermal (vs endodermal body).
- Interureteric ridge (between ureteric orifices) clinically visible on cystoscopy.
- Histological Layers 🧪
- Mucosa: Transitional (urothelium) epithelium (6–8 layers when empty → 2–3 when stretched) + lamina propria (connective tissue with blood vessels, nerves, lymphoid follicles).
- Submucosa (lamina propria continuation): loose connective tissue; allows folding (rugae) when empty.
- Muscularis (Detrusor muscle): Thick smooth muscle in 3 poorly defined layers (inner/outer longitudinal, middle circular) → powerful contraction during voiding.
- Adventitia/Serosa: Outer connective tissue; superior surface covered by visceral peritoneum (serosa).
🩸 Vascular Supply
- Arterial ❤️
- Superior vesical arteries (from internal iliac) → anterosuperior bladder.
- Inferior vesical arteries (males) / vaginal artery (females) → posteroinferior bladder.
- Additional: obturator, uterine, middle rectal arteries.
- Venous 💉
- Vesical venous plexus → internal iliac veins (main drainage).
- Connections to prostatic/uterine/vaginal plexuses → risk of spread in malignancy.
- Lymphatic: Follow arteries → internal iliac → common iliac → para-aortic nodes.
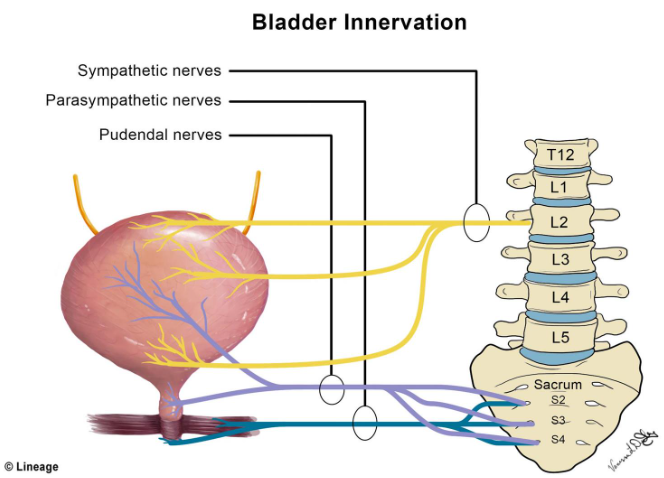
🧠 Neural Supply & Micturition Reflex
| Division | Origin | Target | Effect | Neurotransmitter |
|---|---|---|---|---|
| Sympathetic (storage) | Hypogastric plexus (T10–L2) | Detrusor muscle
Internal urethral sphincter | Relaxes detrusor
Contracts sphincter | Noradrenaline (β₂/β₃ receptors on detrusor, α₁ on sphincter) |
| Parasympathetic (voiding) | Pelvic splanchnic nerves (S2–S4) | Detrusor muscle
Internal urethral sphincter | Contracts detrusor
Relaxes sphincter | Acetylcholine (M₃ receptors) |
| Somatic (voluntary) | Pudendal nerve (S2–S4) | External urethral sphincter (striated muscle) | Voluntary contraction (continence) | Acetylcholine (nicotinic receptors) |
- Storage phase (sympathetic dominance): Low pressure filling (compliance), closed sphincters.
- Micturition reflex:
- Stretch receptors (Aδ/C fibres) in detrusor → pelvic nerves → sacral cord (S2–S4) → pontine micturition centre → cerebral cortex (voluntary control).
- Threshold ~200–400 mL → urge; voluntary relaxation of external sphincter + parasympathetic activation → detrusor contraction + sphincter relaxation.
- Neurogenic bladder: Suprapontine (uninhibited), spinal (detrusor-sphincter dyssynergia), infrasacral (atonic).
🫁 Physiology of the Bladder
- Filling/Storage phase:
- Ureters deliver urine intermittently → bladder fills slowly.
- Detrusor relaxes (sympathetic β₃), sphincters contracted → pressure remains low (<10–15 cm H₂O).
- Capacity: functional 400–600 mL; max ~800–1000 mL before strong urge.
- Voiding phase (micturition):
- Threshold stretch → afferent signals → reflex + voluntary inhibition release.
- Parasympathetic → detrusor contraction (intravesical pressure 40–100 cm H₂O).
- Sphincter relaxation → urine expulsion (~15–25 mL/s flow rate).
- Completion: detrusor relaxes, sphincters close.
🩺 Clinical Relevance
- Urinary incontinence 💦: Stress (pelvic floor weakness), urge (overactive bladder/detrusor instability), overflow (retention), functional (mobility/cognition).
- Urinary retention 🚫: Acute (BPH, drugs, post-op) vs chronic (neurogenic, obstruction) → risk of hydronephrosis, UTI, overflow incontinence.
- Cystitis / UTI 🔥: Bacterial (E. coli), interstitial (painful bladder syndrome), radiation/chemotherapy-induced.
- Bladder cancer 🧬: Transitional cell carcinoma (90%); risk factors: smoking, aromatic amines, schistosomiasis (squamous); painless haematuria most common presentation.
- Neurogenic bladder 🧠: MS, spinal cord injury, diabetic neuropathy → detrusor hyperreflexia/areflexia, dyssynergia → high-pressure retention, reflux nephropathy.
Teaching Point 🩺 Bladder = distensible storage organ (400–600 mL) with transitional epithelium + powerful detrusor. Storage: sympathetic (relax detrusor, contract sphincters). Voiding: parasympathetic (contract detrusor, relax internal sphincter) + voluntary external sphincter relaxation. Trigone = fixed, smooth area (ureteric + urethral orifices). Clinical keys: haematuria → cancer/UTI; retention → overflow incontinence; low compliance → high-pressure damage to kidneys.
📚 References (Feb 2026)
- Gray’s Anatomy 42nd ed. (2020; 2025 online updates).
- Wein AJ et al. Campbell-Walsh Urology (13th ed., 2025).
- EAU Guidelines: Neuro-urology & Incontinence (2025–2026).
- Recent: Bladder mechanosensation & TRP channels (Nature Rev Urol 2025).
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery