
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Goitre ✅
Related Subjects: |Neck Swellings by Triangle |Thyroglossal cyst |Head and Neck Cancers |Triangles of the neck |Cervical Lymphadenopathy |Goitre
🧑⚕️ Pemberton’s sign: Raising both arms above the head causes facial congestion, cyanosis, and respiratory distress due to obstruction of the thoracic inlet by a retrosternal goitre. A key bedside OSCE finding; positive in large substernal or mediastinal thyroid enlargement.
📖 About
- Goitre = enlarged thyroid gland (diffuse or nodular).
- WHO definition: thyroid lobes larger than the terminal phalanx of the patient’s thumb.
- Can be diffuse (uniform enlargement) or nodular (single or multinodular).
- May be euthyroid, hyperthyroid, or hypothyroid depending on aetiology.
⚡ Compression symptoms
- Tracheal compression: dyspnoea, cough, choking sensation, wheeze or stridor 🚨
- Retrosternal extension: pressure symptoms may worsen when lying flat or raising the arms.
- SVC compression: facial plethora, engorged neck/upper chest veins and Pemberton’s sign.
- Recurrent laryngeal nerve involvement: hoarseness or voice change - consider thyroid malignancy until excluded.
- Oesophageal compression: dysphagia or a sensation of food sticking.
⚡ Causes of Goitre
- Physiological: puberty and pregnancy, due to increased thyroid hormone demand.
- Autoimmune: Hashimoto’s thyroiditis and Graves’ disease.
- Iodine-related: iodine deficiency or excess.
- Inflammatory: subacute thyroiditis, including de Quervain thyroiditis.
- Drug-related / goitrogens: 💊 lithium, amiodarone and other goitrogenic agents.
- Smoking: 🚬 associated with thyroid enlargement and Graves’ orbitopathy.
- Nodular thyroid disease: multinodular goitre, solitary thyroid nodule or thyroid cyst.
- Neoplastic: thyroid adenoma or thyroid carcinoma, especially if hard, fixed or rapidly enlarging.
- Genetic / familial: familial goitre or inherited dyshormonogenesis.
- Idiopathic: no clear cause identified.
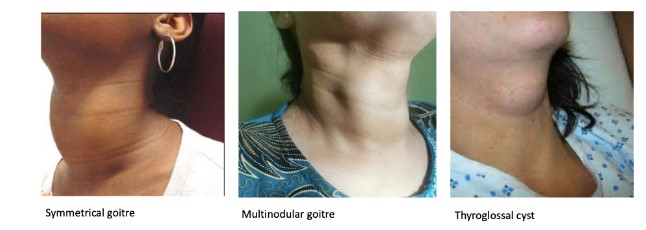
📑 Types of Goitre
- Diffuse non-toxic goitre: uniform thyroid enlargement, usually euthyroid; may cause tracheal or oesophageal compression if large.
- Diffuse toxic goitre: usually due to Graves’ disease; diffuse enlargement with biochemical hyperthyroidism.
- Nodular goitre: one or more discrete nodules; may be benign, cystic, inflammatory or malignant.
- Multinodular goitre: multiple thyroid nodules; may be non-toxic or toxic if autonomous hormone production develops.
- Retrosternal goitre: thyroid enlargement extending below the thoracic inlet; more likely to cause dyspnoea, stridor, dysphagia or SVC-type symptoms.
📏 WHO Grading of Goitre
- Grade 0: Not palpable or visible
- Grade 1: Palpable, not visible in neutral neck; includes small nodules
- Grade 2: Clearly visible swelling in neutral neck
🚩 Malignancy High-Risk Features
- Rapid growth or hard, fixed nodule
- Hoarseness (recurrent laryngeal nerve involvement)
- Cervical lymphadenopathy
- History of head/neck irradiation
- Thyroid cancer in first-degree relative
- MEN2 syndrome / elevated calcitonin
- FDG-PET avidity on incidental imaging
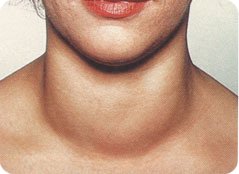
🩺 Clinical Examination
- Inspect from front & behind: neck contour, asymmetry, tracheal deviation.
- Palpate thyroid and cervical lymph nodes; assess nodularity, consistency, tenderness.
- Ask patient to swallow: thyroid moves upwards with swallowing.
- Listen for bruit (Graves’ disease).
- Check voice: hoarseness → recurrent laryngeal nerve compression.
- Assess for compressive symptoms: dyspnoea, dysphagia, stridor.
- Perform Pemberton’s manoeuvre if retrosternal extension suspected.
- Evaluate thyroid function signs: hypo- or hyperthyroid features.
🔬 Investigations
- Bloods: FBC, U&E, CRP (infection or inflammation)
- TFTs: TSH, free T4, T3. Hashimoto: ↑TSH; Graves: ↓TSH, ↑T3/T4
- Autoantibodies: Anti-TPO, Anti-Tg; TSH receptor antibodies for Graves’ disease
- Imaging:
- Ultrasound: first-line for morphology, nodule characterization, FNA guidance
- Radionuclide scan: if TSH suppressed (hot vs cold nodules)
- CT thoracic inlet / MRI: for retrosternal or mediastinal extension; use non-contrast to avoid iodine load if future RAI planned
🔍 FNA Indications (Nodules)
- Suspicious nodule + cervical lymphadenopathy
- High-risk history: ≥5 mm
- Microcalcification: >1 cm
- Solid nodule: >1 cm
- Mixed cystic-solid: >1.5–2 cm
- Spongiform: >2 cm
- Pure cystic: no FNA required
💊 Management (NICE-compliant)
- Rule out malignancy: USS ± FNA
- Observation: small, asymptomatic benign goitres; annual clinical review
- Iodine supplementation: if deficiency suspected (esp. endemic areas)
- Medical therapy:
- Thyroxine suppression rarely used; antithyroid drugs (Carbimazole, Propylthiouracil) for toxic goitre
- Radioactive iodine: indicated for toxic diffuse or multinodular goitre
- Surgery: for suspected malignancy, compressive symptoms, cosmetic concern, or failed medical therapy; total or hemithyroidectomy depending on disease
- Monitor airway and postoperative complications (haematoma, hypocalcaemia, RLN injury)
Cases - Goitre (Thyroid Enlargement)
- Case 1 - Multinodular Goitre with Compressive Symptoms 🦴: 68F, neck swelling, intermittent dysphagia, hoarseness. Irregular nodular thyroid, retrosternal extension, tracheal deviation on CXR. TFTs normal. Management: Surgical thyroidectomy, airway monitoring, histology to exclude malignancy.
- Case 2 - Diffuse Toxic Goitre (Graves’) 🔥: 32F, weight loss, heat intolerance, tremor, palpitations. Smooth diffuse goitre with bruit; exophthalmos, pretibial myxoedema. TFTs: TSH suppressed, T3/T4 elevated; TRAb positive. Management: Antithyroid drugs, β-blockers; consider RAI or surgery if relapse; ophthalmology review.
- Case 3 - Endemic Simple Goitre 🌍: 19F, large painless diffuse thyroid, no eye or compressive signs. Low dietary iodine; TFTs normal. Management: Iodine supplementation, dietary education; surgery if very large or disfiguring.
Teaching Commentary 🧠
Goitre assessment integrates function, structure, and compression. - Diffuse: Graves’ (hyperthyroid), Hashimoto’s (hypothyroid), simple/iodine deficiency (euthyroid). - Nodular: multinodular goitre, solitary nodule (benign vs malignant). Red flags: rapid growth, hard/irregular nodule, cervical lymphadenopathy, hoarseness → FNA ± surgery. NICE-compliant management: targeted investigation, risk stratification, stepwise intervention (observation → medical → RAI → surgery) with monitoring of airway and thyroid function.



| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery