Related Subjects:
|ECG Basics
|ECG Axis
|ECG Analysis
|ECG LAD
|ECG RAD
|ECG Low voltage
|ECG Pathological Q waves
|ECG ST/T wave changes
|ECG LBBB
|ECG RBBB
|ECG short PR
|ECG Heart Block
|ECG Asystole and P wave asystole
|ECG QRS complex
|ECG ST segment
|ECG: QT interval
|ECG: LVH
|ECG RVH
|ECG: Bundle branch blocks
|ECG Dominant R wave in V1
|ECG Acute Coronary Syndrome
|ECG Crib sheets
📌 About
- The ST segment represents the period between ventricular depolarisation and repolarisation.
- It is normally isoelectric (flat) and shifts up or down when the myocardium is injured, inflamed, or stressed.
- Careful interpretation is vital as ST changes can indicate life-threatening cardiac pathology.



⬆️ ST Elevation
- Physiological “high take-off”: Fixed, benign elevation in V1–V3 (young healthy adults).
- Acute MI 🚑: ≥1 mm in 2 contiguous limb leads OR ≥2 mm in 2 chest leads. Often convex “tombstone” with reciprocal depression elsewhere.
- Pericarditis/Myocarditis ❤️🔥: Widespread, saddle-shaped, concave ST elevation (spares aVR, V1).
- LBBB: ST elevation can accompany abnormal conduction (use Sgarbossa criteria if MI suspected).
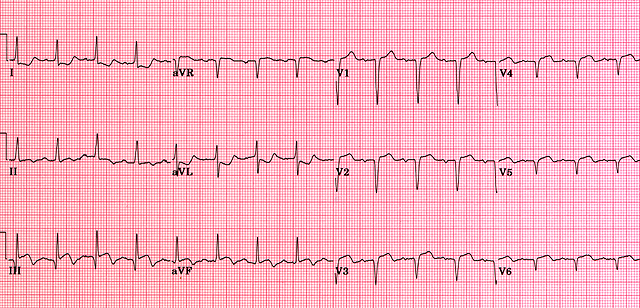
- LVH strain: ST elevation in right chest leads; usually with deep S waves and T inversion elsewhere.
- Brugada Syndrome ⚡: Coved ST elevation in V1–V3 (“shark fin” morphology); risk of sudden cardiac death.
- Coronary Spasm (Prinzmetal’s angina): Transient ST elevation resolving with nitrates.
- LV Aneurysm (post-MI scar): Persistent ST elevation without reciprocal changes.
⬇️ ST Depression
- Myocardial Ischaemia 🫀: Horizontal or down-sloping ST depression (≥1 mm) in V4–V6 = significant. Severity: Down-sloping > Flat > Up-sloping.
- LVH strain pattern: ST depression with asymmetrical T inversion in lateral leads.
- Digoxin effect 💊: “Reverse tick” scooped ST depression – classic exam favourite.
- Electrolyte disturbance: Hypokalaemia causes ST depression + U waves.
- Non-cardiac causes: Hyperventilation may mimic transient depression.
🚑 Immediate Action
- Suspected ACS: Treat as emergency if chest pain + ST changes.
- Give O₂ (if hypoxaemic), GTN spray, Aspirin 300 mg.
- Call 999 (UK) for rapid transfer to PCI centre if STEMI or ACS equivalent.
- Always compare with old ECGs to distinguish chronic vs acute changes.
