Related Subjects:
|Chest X Ray Interpretation
|Chest X Ray Collection
📖 Introduction
- Postero-anterior (PA): Standard view. Patient stands facing the plate, scapulae rotated out. Best quality, less cardiac magnification.
- Antero-posterior (AP): Portable view in sick patients. Heart shadow appears larger, often poorer inspiration/quality.
- Lateral (LAT): Used to assess posterior mediastinum, retrosternal and retrocardiac areas. CT is usually superior for localisation.
🧭 Technical Quality Checks
- ✅ Patient details: name, DOB, date/time of CXR.
- ✅ Projection: PA or AP? (important for heart size).
- ✅ Rotation: medial clavicles equidistant from spinous processes.
- ✅ Inspiration: ≥6 anterior ribs above diaphragm.
- ✅ Penetration: vertebrae just visible behind heart.
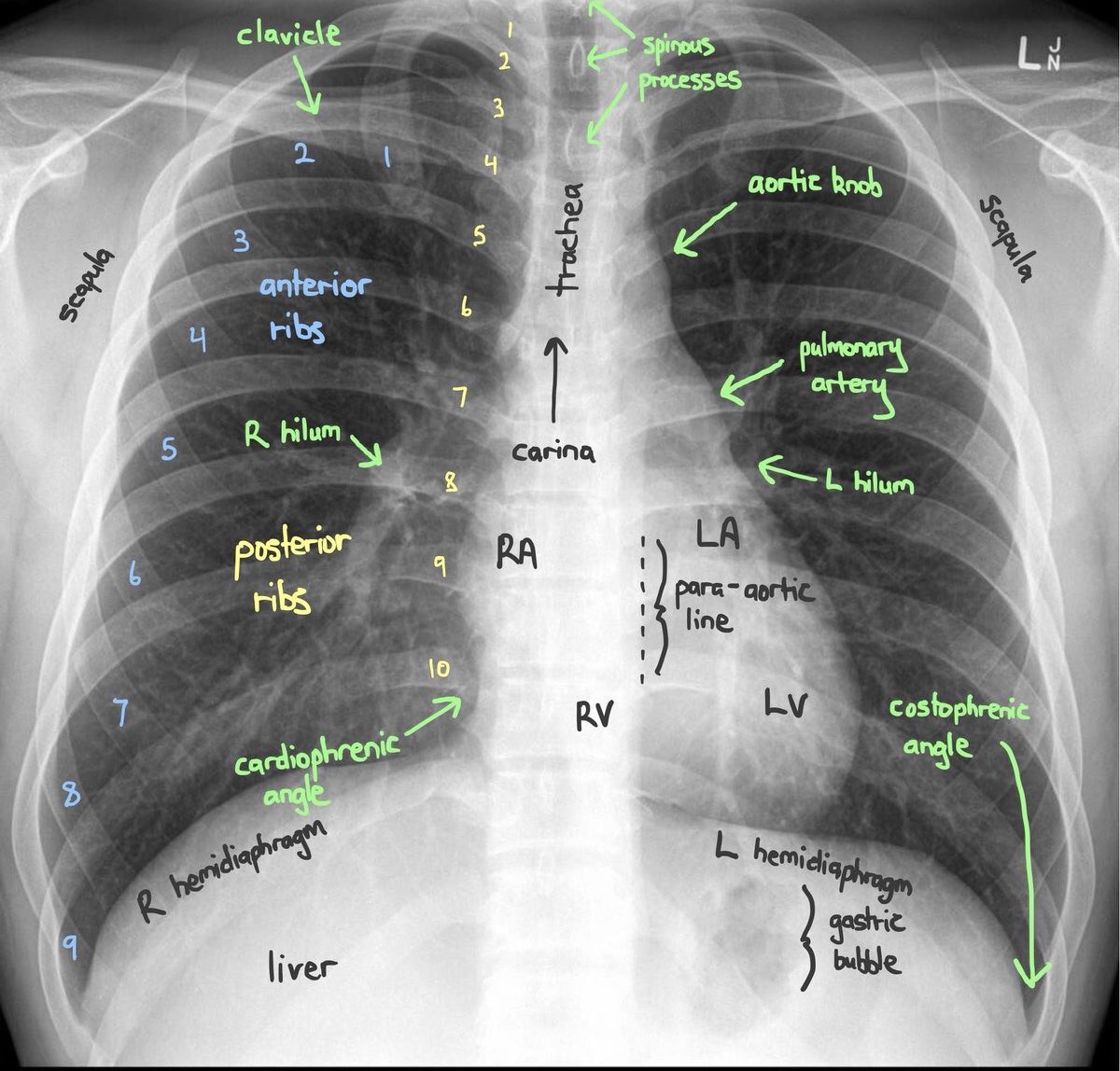
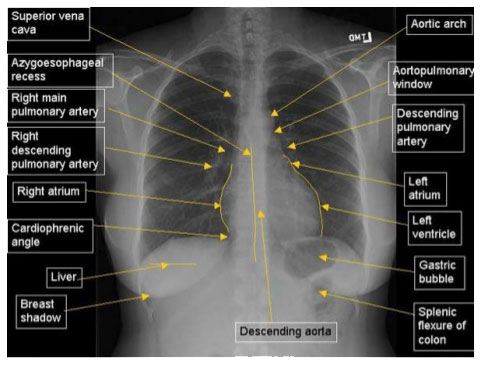
🫁 Normal Anatomy & Landmarks
📊 Stepwise Interpretation of a CXR (ABCDE)
- 📝 A – Airway
– Trachea central? (deviation = effusion, pneumothorax, collapse, mass).
– Carina and main bronchi visible.
- 🦴 B – Bones & Soft Tissues
– Ribs, clavicles, scapulae, vertebrae → fractures, lytic lesions, metastases.
– Look for cervical rib, lytic deposits.
– Breast shadows present? Absent shadow = mastectomy.
- ❤️ C – Cardiac & Mediastinum
– Heart size: cardiothoracic ratio >0.5 = cardiomegaly (only valid PA).
– Aortic knuckle, pulmonary artery, mediastinal width.
– Situs? (stomach bubble, cardiac apex).
- ⬇️ D – Diaphragm
– Right higher than left.
– Sharp costophrenic angles? Blunting = pleural effusion.
– Free air under diaphragm = perforated viscus.
– Gastric bubble under left diaphragm.
- 🌫️ E – Effusions / Equal Lung Fields
– Compare both lungs side by side.
– Peripheral absence of markings = pneumothorax.
– Opacities = consolidation, collapse, mass, interstitial patterns.
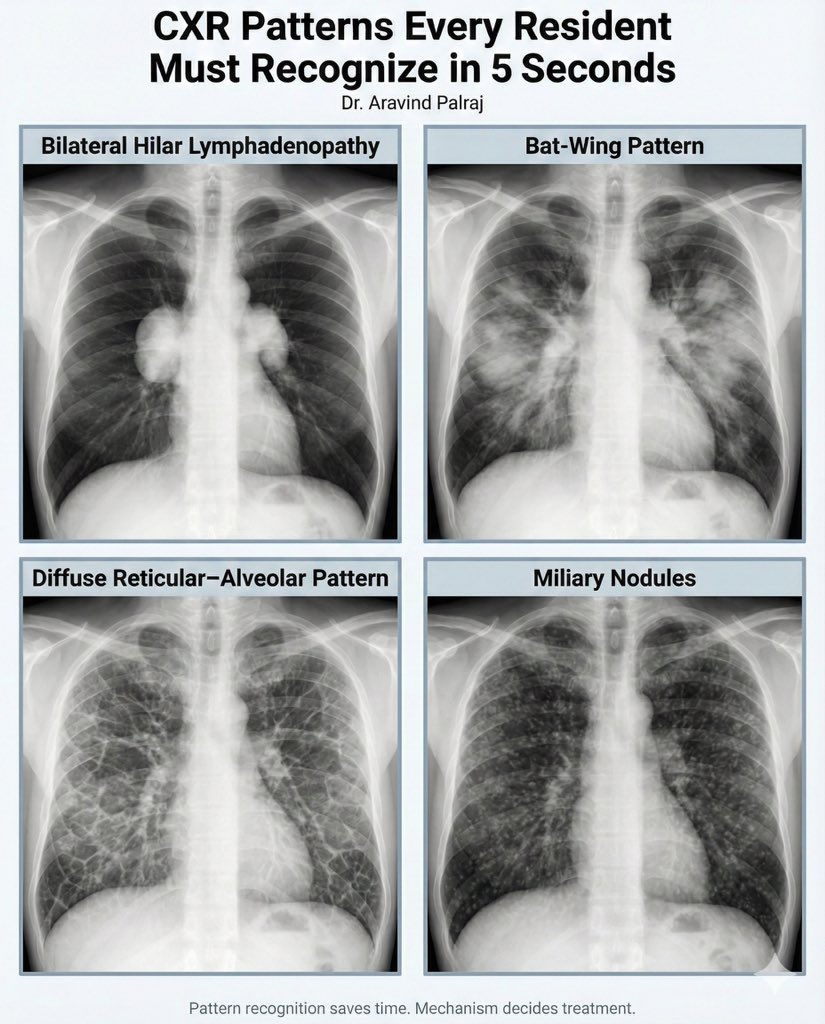
– “Bat’s wing” shadowing = pulmonary oedema.
- 🔌 F – Foreign Bodies / Lines
– NG tube → below diaphragm, midline.
– Central line → tip at cavo-atrial junction.
– ETT tube → 3–5 cm above carina.
– Pacemakers, chest drains, prosthetic valves.
- 🧭 G – Great Vessels & Hila
– Left hilum slightly higher than right.
– Unilateral enlargement → TB, cancer, lymphoma.
– Bilateral hilar enlargement → sarcoid, TB, lymphoma.
- 🔍 H – Hidden Areas (Final Sweep)
– Apices: small PTX, Pancoast tumour.
– Behind the heart: pneumonia, hiatus hernia.
– Bones again: subtle fractures, mets.
– Soft tissues: subcutaneous emphysema.
📌 Common Pathologies on CXR
- 🌫️ Lobar consolidation (pneumonia)
- 💨 Pneumothorax (loss of markings)
- 💦 Pulmonary oedema (bat’s wing)
- 🌪️ Pleural effusion (meniscus sign)
- 📉 Lobar collapse (volume loss, mediastinal shift)
- 🫀 Cardiomegaly (CT ratio >0.5 PA)
- 🦠 TB (upper zone cavitation, fibrosis, hilar nodes)
- 🎯 Lung mass / Pancoast tumour
- 📍 NG tube / central line / pacemaker position
⚠️ “Normal” CXR in Sick Patients
- Asthma, COPD
- Pulmonary embolism
- Early pneumonia
- Pneumocystis pneumonia
- ARDS (may evolve)
- DKA with Kussmaul breathing (normal CXR)
🚨 Things Commonly Missed
- Apices: small pneumothorax, Pancoast tumour.
- Retrocardiac: pneumonia, hiatus hernia, vertebral lesions.
- Cardiac: valve calcifications.
- Skeletal: cervical rib, subtle mets.
- Gas: pneumoperitoneum, pneumomediastinum.
- Soft tissue: absent breast shadow (mastectomy).
🌿 Fibrosis Patterns
- Upper zone: TB, sarcoid, silicosis, ankylosing spondylitis, hypersensitivity pneumonitis.
- Lower zone: idiopathic pulmonary fibrosis, asbestosis, connective tissue disease (RA, SLE, SSc), drugs (amiodarone, bleomycin, methotrexate).
🔎 Classic Exam Findings
- 🫧 Bilateral hilar lymphadenopathy → sarcoid, TB, lymphoma.
- 🫀 Opaque hemithorax → effusion, consolidation, collapse, pneumonectomy.
- 🕳️ Cavitating lesion → TB, abscess, squamous carcinoma, septic emboli.
- ⚡ Pneumothorax → absent markings, pleural edge.
- 💦 Pulmonary oedema → peri-hilar “bat’s wing” shadowing.
💡 Teaching Pearls:
– Always start with technical quality before pathology.
– Use a systematic approach (A → H).
– Comment on tubes and devices.
– A “normal CXR” does not exclude serious pathology (PE, asthma, early pneumonia, PCP).