
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Benign Prostatic Hyperplasia✅
Related Subjects: |Urothelial tumour s |Haematuria |Acute Urinary Retention |Anuria and Oliguria |Bladder cancer |Renal cell carcinoma |Benign Prostatic Hyperplasia |IgA nephropathy |Prostate Cancer |Henoch-Schonlein purpura |Glomerulonephritis
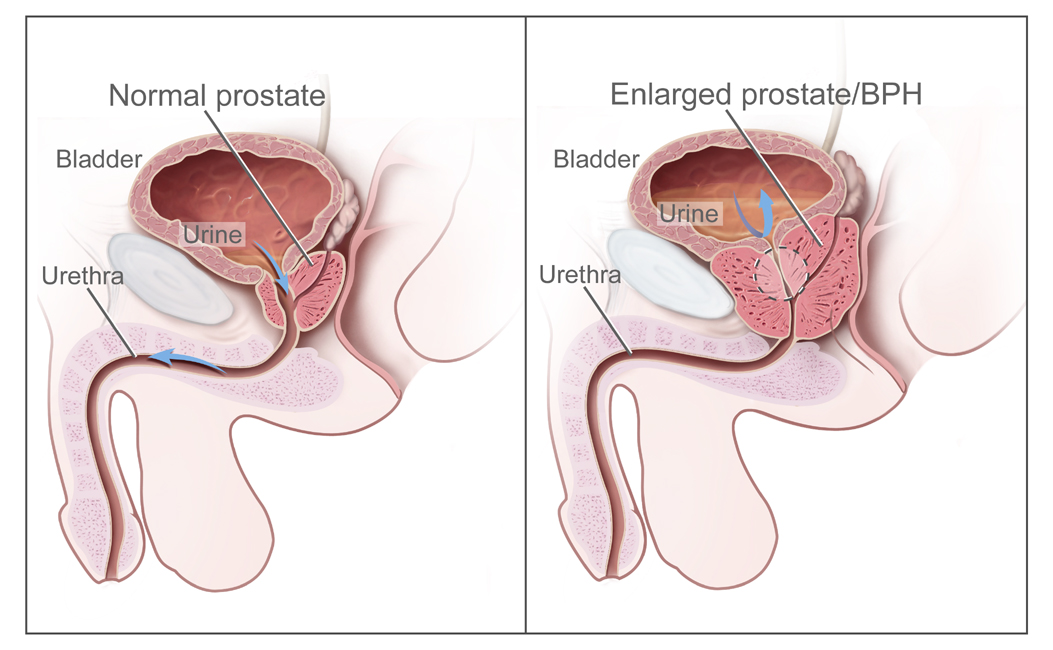
🔵 Benign Prostatic Hyperplasia (BPH) / Male LUTS usually affects the peri-urethral (transition) zone of the prostate. 📏 Importantly, prostate size does not always correlate with urinary obstruction.
📌 About
- Male LUTS may arise from BPH, detrusor overactivity, impaired contractility, or mixed mechanisms 🚻.
- Prostate size alone is not a reliable predictor of obstruction 🚫.
- Assessment guided by IPSS score, DRE, PSA, and symptom diary aligns with NICE CG97 guidance.
🧬 Pathology
- Represents hyperplasia (increase in cell number) rather than hypertrophy.
- Confined mainly to the peri-urethral (transition) zone.
- Chronic obstruction → detrusor hypertrophy → trabeculation → impaired emptying.
👨 Clinical Features
- Common in men >50 yrs; prevalence: Black > White > Asian.
- Voiding symptoms: weak stream, hesitancy, terminal dribbling 🚽.
- Storage symptoms: frequency, urgency, nocturia ⏰.
- Incomplete emptying → chronic retention with large bladder.
- Exam: smooth enlarged prostate, palpable bladder.
⚠️ Complications
- Acute urinary retention (may be worsened by drugs ❗ e.g., anticholinergics, antihistamines, antidepressants).
- Recurrent UTIs 🦠.
- Hydroureter, hydronephrosis, renal impairment 🩸.
- Bladder calculi & infection.
🔍 Investigations
- Symptom assessment: IPSS or AUASS score.
- Urinalysis (MSU if positive); haematuria → rule out malignancy 🔎.
- Bloods: U&E, FBC, PSA (interpret carefully: ↑ in BPH, infection, recent catheterisation).
- Post-void residual (PVR) via bladder scan or ultrasound; >150 mL may indicate impaired emptying.
- Frequency-volume chart (2–3 days) to assess LUTS patterns.
- Abdominal ultrasound: kidney size, hydronephrosis, bladder wall changes.
- Flexible cystoscopy if haematuria, obstruction, or uncertain diagnosis.
- Urodynamics: only in complex cases (neurogenic bladder or failed prior surgery).
💡 General Lifestyle Advice
- Limit alcohol 🍺, caffeine ☕, and evening fluids.
- Avoid decongestants/antihistamines as they worsen retention.
- Bladder training: urinate regularly (every 4–6 hrs), double voiding helps empty residual urine.
- Maintain healthy weight & stay active 🏃 – reduces retention risk.
- Keep warm 🧥 – cold exposure may trigger urinary retention.
💊 Medical Management (NICE CG97)
- Alpha-blockers (Tamsulosin, Alfuzosin): relax smooth muscle → rapid symptom relief (days–weeks). ⚠️ SE: postural hypotension, dizziness.
- 5-alpha reductase inhibitors (Finasteride, Dutasteride): shrink prostate gradually (3–6 months), reduce long-term risk of retention/surgery. ⚠️ SE: retrograde ejaculation, reduced libido.
- Combination therapy: alpha-blocker + 5-ARI for large prostates or severe symptoms.
- Anticholinergics (Oxybutynin): for storage symptoms; caution in elderly/frail (delirium risk).
- Mirabegron: β3 agonist alternative for overactive bladder; SE: hypertension.
🧴 Catheterisation & TWOC
- Acute retention: catheterise + start alpha-blocker → trial without catheter (TWOC) in 2–7 days.
- If TWOC fails: intermittent self-catheterisation or long-term catheter (urethral/suprapubic).
- Severe chronic retention (>800–1000 mL) may require long-term catheterisation.
📤 Indications for Urology Referral
- Suspicion of malignancy (hard nodular prostate, elevated PSA).
- Obstructive uropathy: AKI, raised urea/creatinine.
- Large bladder, recurrent retention, or hydronephrosis.
- Rapidly worsening LUTS or failure of medical therapy.
🔪 Surgical Options
- TURP: gold standard for moderate prostate size; removes obstructive tissue via resectoscope. SE: bleeding, TURP syndrome, clot retention, stricture, retrograde ejaculation, incontinence.
- HoLEP (Holmium Laser Enucleation): preferred for large prostates; less bleeding, durable results, shorter catheter time.
- Minimally invasive: UroLift, Rezūm (for select patients prioritising ejaculation preservation).
- Open prostatectomy: for very large prostates or complex anatomy.
Case 1 – Mild Symptoms
58-year-old with daytime frequency and nocturia ×2. DRE normal, PSA normal, PVR 40 mL. Implement lifestyle modifications. If symptoms persist, start an alpha-blocker and review in 4–6 weeks.
Case 2 – Moderate Symptoms, Enlarged Prostate
66-year-old, IPSS 18, smooth prostate, PSA 2.4 µg/L, volume ~45 mL, PVR 120 mL. Start tamsulosin and 5-alpha-reductase inhibitor. Consider mirabegron if storage symptoms persist and PVR is low.
Case 3 – Acute Urinary Retention
74-year-old unable to void. Catheterise, start alpha-blocker, check for UTI or culprit meds. Plan TWOC in 2–7 days. If failure or complications, refer for surgery (TURP/HoLEP) depending on prostate size and patient fitness.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery