Related Subjects: Asthma
|Pleural effusion
|Exacerbation of COPD
|Pulmonary Embolism
|Cardiogenic Pulmonary Oedema
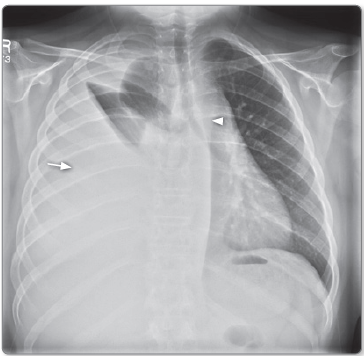
|Pneumothorax
💡 Key Point: The “meniscus” on CXR is a visual illusion caused by thoracic shape – not a true meniscus.
💉 Diagnostic tap: 20 mL syringe + 21G needle → send fluid for protein/LDH, cell count, culture (inc. TB), and cytology.
⚠️ Large-volume rapid drainage risks re-expansion pulmonary oedema → always drain slowly with monitoring.
📖 About
- 🫁 Pleural effusion = fluid in pleural space → impaired lung expansion + breathlessness.
- 🔍 Suggests underlying lung/pleural/systemic disease (infection, malignancy, systemic illness).
🔄 Types
- 💧 Pleural Effusion: Fluid in pleural space.
- 🌬️ Pneumothorax: Air in pleural space.
- 🟢 Empyema: Pus in pleural space (often post-infection).
- 🩸 Haemothorax: Blood, usually trauma/malignancy.
- 🥛 Chylothorax: Milky lymph (thoracic duct injury/malignancy).
🧪 Aetiology
- Causes: inflammation, malignancy, ↑ permeability, or osmotic imbalance.
- 🔎 Classified by Light’s Criteria → Exudates (high protein) vs Transudates (low protein).
🩺 Clinical (detectable if >500 mL)
- 😮 Progressive breathlessness.
- ⚡ Pleuritic chest pain (esp. inflammatory).
- 📉 Reduced chest movement on affected side.
- 🔨 Stony dull percussion.
- ➡️ Mediastinal shift/tracheal deviation in large effusions.
- 🔇 ↓ breath sounds + vocal resonance over fluid.
- 🎶 Bronchial breathing above fluid level.
📊 Light’s Criteria – Exudate if ≥1 present
- Protein ratio (pleural/serum) > 0.5
- LDH ratio (pleural/serum) > 0.6
- Pleural LDH > ⅔ upper serum LDH normal

🔍 Classical Findings by Cause
- 🎗️ Cancer: Serous/bloody exudate. Cytology/biopsy may show malignant cells.
- ❤️ Heart Failure: Transudate, straw-coloured. Responds to diuretics. BNP↑.
- 🦠 Tuberculosis: Amber fluid, lymphocytosis, exudative. ADA↑.
- 🫀 Pulmonary Embolism: Clear/blood-stained. Exudate or transudate.
- 🦴 Rheumatoid: Turbid, high lymphocytes, low glucose, cholesterol crystals.
- 🌸 SLE: Serous, lymphocytic. ANA/anti-DNA positive.
- 🔥 Pancreatitis: Bloody/serous, amylase↑.
- 🥛 Chylothorax: Milky (chylomicrons present).
📌 Causes Using Light’s Criteria
- Exudates: (high protein/LDH)
- Bacterial pneumonia, TB, abscess, fungal.
- Malignancy: carcinoma, lymphoma, mesothelioma.
- Autoimmune: RA, SLE, vasculitis.
- Pancreatitis, oesophageal rupture.
- Radiation/asbestos lung injury.
- Transudates: (low protein/LDH)
- Heart failure, nephrotic syndrome, cirrhosis.
- Hypoalbuminaemia, peritoneal dialysis.
- Urinothorax (urinary obstruction).
- CSF leak into pleural space.
💉 Therapeutic Tap
- Indicated if breathless/unclear cause. Avoid in HF unless diuretic-resistant.
- Relieves symptoms + diagnostic yield.
- 🔎 Use small-bore (10–14F) drain, ideally US-guided.
- ⚠️ Drain slowly & intermittently → prevent re-expansion pulmonary oedema.
- 🟢 Empyema → antibiotics + larger drain ± intrapleural fibrinolytics.
📚 References
4 Clinical Cases - Pleural Effusion 🌊🫁
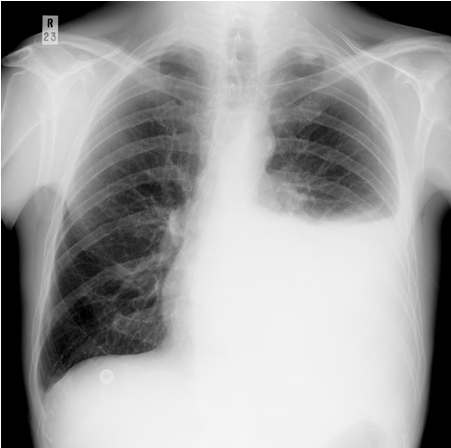
- Case 1 - Heart failure (transudate) ❤️: A 72-year-old man with worsening orthopnoea and ankle swelling. CXR: bilateral, symmetric pleural effusions with blunting of costophrenic angles. BNP elevated. Teaching: Transudative effusions from raised hydrostatic pressure (HF, nephrotic syndrome, cirrhosis). Treat underlying cause + diuretics; thoracocentesis if symptomatic.
- Case 2 - Pneumonia (parapneumonic effusion) 🦠: A 46-year-old woman with fever, pleuritic chest pain, and productive cough. CXR: left lower lobe consolidation with associated effusion. Pleural fluid: exudate, neutrophil-predominant, pH 7.1. Teaching: Exudates arise from inflammation/infection. Low pH and low glucose suggest complicated effusion/empyema → chest drain often required.
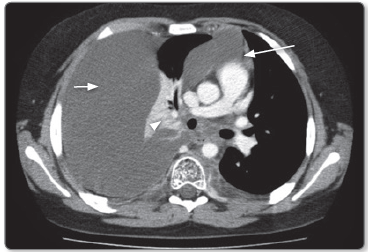
- Case 3 - Malignancy (exudate) 🎗️: A 65-year-old woman with weight loss and dyspnoea. Ex-smoker, history of breast cancer. CXR: right-sided large effusion, mediastinal shift to opposite side. Pleural tap: exudate with malignant cells. Teaching: Malignant effusions often recur. Options: repeated aspiration, indwelling pleural catheter, or talc pleurodesis for palliation.
- Case 4 - Tuberculous effusion 🧫: A 29-year-old man recently arrived from South Asia with fever, night sweats, and pleuritic chest pain. CXR: unilateral pleural effusion, no obvious consolidation. Pleural aspirate: straw-coloured exudate, lymphocyte-rich, ADA elevated. Teaching: TB effusions are usually unilateral, lymphocytic exudates. Diagnosis via pleural biopsy or PCR. Requires full anti-TB therapy.
