Related Subjects:
|Status Epilepticus (Epilepsy)
|Coma management
|Lorazepam
|Phenytoin
|Levetiracetam
|Epilepsy - General Management
|Epilepsy in Pregnancy
|First Seizure
|Carotid Sinus Syncope
|Brain tumour s
|Astrocytoma
|Brain Metastases
ℹ️ About
- ⚡ A first seizure has an estimated 8–10% lifetime risk of occurrence.
- 📊 Around 3% progress to epilepsy (defined as ≥2 unprovoked seizures >24h apart).
- 🚨 Always consider reversible causes (metabolic, structural, toxic, infectious) before diagnosing epilepsy.
🧬 Aetiology
- 🧠 Prior ischaemic stroke
- 🩸 Intracranial haemorrhage
- 🦠 CNS infections (e.g., meningitis, HSV encephalitis)
- 🤕 Traumatic brain injury
- 🧬 Progressive multifocal leukoencephalopathy (PML)
- 🎗️ Brain tumours
- 🧩 Alzheimer’s disease
- 🔄 Autoimmune conditions (e.g., autoimmune encephalitis)
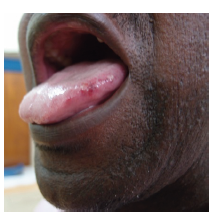
Lateral Tongue Bite compatible with seizure
💊 Drugs That Can Cause Seizures
- Antibiotics: Quinolones, Penicillins, Isoniazid
- Anticholinesterases: Organophosphates, Physostigmine
- Antidepressants: Tricyclics, SSRIs, heterocyclics
- Antihistamines: First-gen and some second-gen agents
- Antipsychotics: Phenothiazines, Butyrophenones, Atypicals
- Chemotherapeutics: Etoposide, Ifosfamide, Cisplatin
- Immunosuppressants: Cyclosporine, Tacrolimus
- Hypoglycaemics: Insulin, sulphonylureas
- Electrolyte disturbance: Hypo-osmolar IV solutions
- Lithium: Toxic levels
- Local Anaesthetics: Bupivacaine, Lidocaine, Procaine
- Methylxanthines: Theophylline, Aminophylline
- Narcotics: Fentanyl, Meperidine, Pentazocine
- Psychoactive drugs: PCP, Cocaine, Amphetamines, Ecstasy (MDMA)
🧾 Clinical Considerations
- 📌 Half of “first seizures” may represent undiagnosed epilepsy with prior minor events.
- 👶 Ask about childhood seizures, febrile convulsions, or developmental issues.
- 🍷 Screen for alcohol or recreational drug use (withdrawal and intoxication common triggers).
- ♀️ Consider catamenial epilepsy (menstrual cycle–related seizures).
🔎 Investigations
- 🩸 Bloods: FBC, U&E, LFTs, Glucose, Calcium, Phosphate, ALP, TFTs
- ❤️ ECG (rule out arrhythmia mimics); consider CXR if aspiration suspected
- 🖥️ Imaging: CT head (if acutely unwell/obtunded); outpatient MRI preferred
- ⚡ EEG: outpatient test to detect epileptiform discharges
📊 Differential Diagnosis
- 💫 Syncope (with anoxic jerks mimicking seizure)
- 🎭 Psychogenic non-epileptic seizures (PNES)
- ⬇️ Hypoglycaemia
- ⬇️ Hypocalcaemia, hyponatraemia
- 🫀 Arrhythmias
💊 Management
- ✅ If patient recovers fully in ED: discharge with safety-netting + seizure advice
- 🚫 Advise not to drive until cleared by DVLA guidance and a neurologist
- 🛡️ Avoid high-risk activities (ladders, swimming alone, operating heavy machinery)
- 👨👩 Stay with a responsible adult for first 48–72h; call 999 if seizures recur
- 🍷 Advise abstinence/reduction in alcohol
- 📅 Urgent neurology referral: specialist review within 2 weeks
- Low-risk patients: (normal neuro exam, MRI & EEG) → recurrence risk ≈ 35% in 5 years → usually no treatment
- High-risk patients: (neurological deficits, abnormal MRI or EEG) → recurrence risk ≈ 70% → usually start anti-seizure medication
📌 UK Practice Tip: DVLA guidance requires at least 6 months off driving after a first seizure (12 months if high recurrence risk), depending on neurologist assessment.
📚 References
