
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Resuscitation - Advanced Life Support Cardiac Arrest
Related Subjects: |Adrenaline/Epinephrine |Atropine |Adult Resus:Acute Anaphylaxis |Adult Resus:Basic Life Support |Adult Resus: Advanced Life Support |Adult Resus: Obstetric Cardiac Arrest |Newborn/Child Resus: All |Acute Hypotension |Cardiogenic shock |Distributive Shock |Hypovolaemic or Haemorrhagic Shock |Obstructive Shock |Septic Shock and Sepsis |Shock (General Assessment) |Toxic Shock Syndrome |Resus:Bradycardia |Resus:Tachycardia |Resus:Hyperkalaemia |Resus:Post Resuscitation Algorithm |Resus:Acute Severe Asthma |Resus:Acute Haemorrhage
🚨 Advanced Life Support (ALS) — Adult Cardiac Arrest
❤️🔥 Core idea: ALS builds on high-quality BLS. The priorities are continuous effective CPR, early defibrillation for VF/pulseless VT, adrenaline at the correct point in the algorithm, and active treatment of reversible causes.
⚡ Rhythm first determines the pathway: shockable = VF / pulseless VT; non-shockable = PEA / asystole.
🔄 During CPR
- Ensure high-quality CPR: rate 100–120/min, depth 5–6 cm, full recoil, minimal interruptions.
- Plan actions before interrupting CPR: rhythm check, shock delivery, airway, drugs and role allocation.
- Give oxygen and ventilate effectively.
- Consider an advanced airway and use continuous waveform capnography if available.
- Once an advanced airway is in place, continue chest compressions without pausing for ventilation.
- Ventilate at about 10 breaths/min once an advanced airway is in place; avoid hyperventilation.
- Obtain IV access; use intraosseous access if IV access is difficult or delayed.
- Give drugs according to shockable or non-shockable algorithm.
- Actively look for and treat reversible causes: 4 Hs and 4 Ts.
- Use capnography to confirm tracheal tube placement and to monitor CPR quality. A sudden rise in ETCO₂ may suggest ROSC.
⚡ Cardiac Arrest Rhythms
| Rhythm group | Rhythms | Key treatment |
|---|---|---|
| Shockable |
|
Defibrillation + CPR + adrenaline after 3rd shock + amiodarone after 3rd shock. |
| Non-shockable |
|
CPR + adrenaline as soon as IV/IO access is available + treat reversible causes. |
⚡ Shockable Arrest: VF / Pulseless VT
⚡ VF and pulseless VT need defibrillation. The most important intervention is rapid shock delivery with minimal interruption to chest compressions.
- Start CPR immediately while the defibrillator is attached.
- Confirm rhythm during a brief pause: VF or pulseless VT.
- Charge defibrillator while compressions continue if safe to do so.
- Deliver shock: commonly 150–200 J biphasic for the first shock, then escalate according to defibrillator guidance/local policy.
- Immediately resume CPR for 2 minutes after the shock.
- Do not check rhythm or pulse immediately after the shock unless the patient shows signs of life.
- After 2 minutes, pause briefly for rhythm check.
- If VF/pVT persists, give a second shock and resume CPR for 2 minutes.
- If VF/pVT persists at the next check, give a third shock and resume CPR immediately.
- After the third shock, give:
- Adrenaline 1 mg IV/IO
- Amiodarone 300 mg IV/IO
- Continue cycles of 2 minutes CPR → rhythm check → shock if indicated.
- Repeat adrenaline 1 mg IV/IO every 3–5 minutes, usually on alternate cycles.
- If VF/pVT persists after the fifth shock, give amiodarone 150 mg IV/IO.
- If ROSC occurs, start post-resuscitation care.
🧊 Safe Defibrillation
- Ensure oxygen is not flowing directly across the chest during shock delivery.
- Announce clearly: “Stand clear”.
- Visually check that nobody is touching the patient, bed or trolley.
- Deliver the shock. Restart CPR immediately after the shock.
🚫 Non-Shockable Arrest: PEA / Asystole
🚫 In PEA and asystole, defibrillation is not indicated. Survival depends on high-quality CPR, early adrenaline, and finding a reversible cause.
- Start CPR immediately: 30 compressions : 2 breaths until an advanced airway is in place.
- Attach monitor/defibrillator and confirm rhythm.
- Check for signs of life and pulse only if rhythm appears compatible with output.
- Give adrenaline 1 mg IV/IO as soon as vascular access is obtained.
- Continue CPR for 2 minutes. Recheck rhythm after 2 minutes.
- If still PEA/asystole, continue CPR and repeat adrenaline 1 mg every 3–5 minutes.
- If VF/pulseless VT appears, change immediately to the shockable rhythm algorithm.
- If ROSC occurs, start post-resuscitation care.
🫀 PEA: Important Point
- PEA means organised electrical activity without a palpable pulse or effective cardiac output.
- Some patients have mechanical activity detectable on ultrasound but no effective circulation.
- Common reversible causes include hypovolaemia, hypoxia, tension pneumothorax, tamponade, massive PE, toxins and severe electrolyte disturbance.
- Bedside ultrasound may help identify reversible causes, but should not cause prolonged pauses in CPR.
📉 Asystole: Important Point
- Check the ECG carefully: confirm leads are attached, gain is appropriate and rhythm is not fine VF.
- True asystole is a non-shockable rhythm.
- Do not attempt defibrillation for true asystole.
- If P waves are present with no QRS complexes, consider ventricular standstill; pacing may be considered with expert help.
- There is no role for pacing in true asystole.
🔁 Reversible Causes: 4 Hs and 4 Ts
| 4 Hs | Treatment clues |
|---|---|
| Hypoxia | Airway manoeuvres, oxygen, ventilation, treat asthma/COPD/pneumonia/aspiration. |
| Hypovolaemia | Fluids, blood products, control haemorrhage, consider sepsis/dehydration/trauma. |
| Hypo-/hyperkalaemia and metabolic disturbance | Check blood gas/U&Es; treat hyperkalaemia with calcium, insulin-glucose and other local protocol measures. |
| Hypothermia | Measure temperature, rewarm, modify resuscitation according to severity. |
| 4 Ts | Treatment clues |
| Thrombosis — coronary | Consider acute MI; urgent cardiology/PCI pathway after ROSC or during refractory arrest in selected systems. |
| Thrombosis — pulmonary | Consider massive PE; thrombolysis may be considered if PE strongly suspected. |
| Tension pneumothorax | Clinical diagnosis; immediate decompression if suspected. |
| Tamponade | Consider trauma, malignancy, post-procedure; urgent drainage/surgical help. |
| Toxins | Consider opioids, tricyclics, beta-blockers, calcium-channel blockers, digoxin and local poisons advice. |
💊 ALS Drugs — Adult Cardiac Arrest
| Drug | Dose | When used | Notes |
|---|---|---|---|
| Adrenaline | 1 mg IV/IO |
|
Flush after administration and continue CPR. |
| Amiodarone | 300 mg IV/IO | After 3rd shock in refractory VF/pulseless VT. | Give during CPR after shock delivery. |
| Amiodarone | 150 mg IV/IO | After 5th shock if VF/pulseless VT persists. | Follow local policy for dilution/administration. |
| Lidocaine | Specialist/local protocol dosing | Alternative antiarrhythmic if amiodarone is unavailable or unsuitable. | Do not give lidocaine if amiodarone has already been given unless expert advice. |
| Magnesium sulfate | Usually 2 g IV for Torsades de pointes or suspected hypomagnesaemia. | Not routine for all cardiac arrests. | |
| Calcium chloride / gluconate | Follow local hyperkalaemia protocol | Hyperkalaemia, hypocalcaemia, calcium-channel blocker toxicity. | Protects myocardium in hyperkalaemia. |
| Sodium bicarbonate | Specialist/local protocol dosing | Severe hyperkalaemia, tricyclic antidepressant overdose, selected severe acidosis. | Not routine in cardiac arrest. |
🫁 Airway and Ventilation During ALS
- Start with simple airway manoeuvres and bag-valve-mask ventilation.
- Use supraglottic airway or tracheal intubation only if trained and it does not interrupt compressions.
- Confirm tracheal tube placement with waveform capnography.
- Once advanced airway is in place, give continuous chest compressions with ventilation about 10 breaths/min.
- Avoid excessive ventilation because it reduces venous return and cardiac output during CPR.
🫀 Post-Resuscitation Care After ROSC
- Use ABCDE reassessment.
- Maintain oxygenation and ventilation; avoid severe hypoxia and avoid unnecessary hyperoxia.
- Obtain 12-lead ECG and consider urgent coronary reperfusion if STEMI or high suspicion of coronary occlusion.
- Treat hypotension with fluids, vasopressors/inotropes and senior/ICU support.
- Check glucose, temperature, electrolytes and arterial/venous blood gas.
- Identify and treat the cause of arrest.
- Admit to an appropriate monitored setting, usually ICU or coronary care depending on cause.
🦠 Infection / Aerosol Precautions
- Use appropriate PPE according to local infection-control policy.
- Do not use outdated COVID-specific algorithms as the default ALS pathway.
- If high-risk respiratory infection is suspected, prioritise staff safety while minimising delay to CPR and defibrillation.
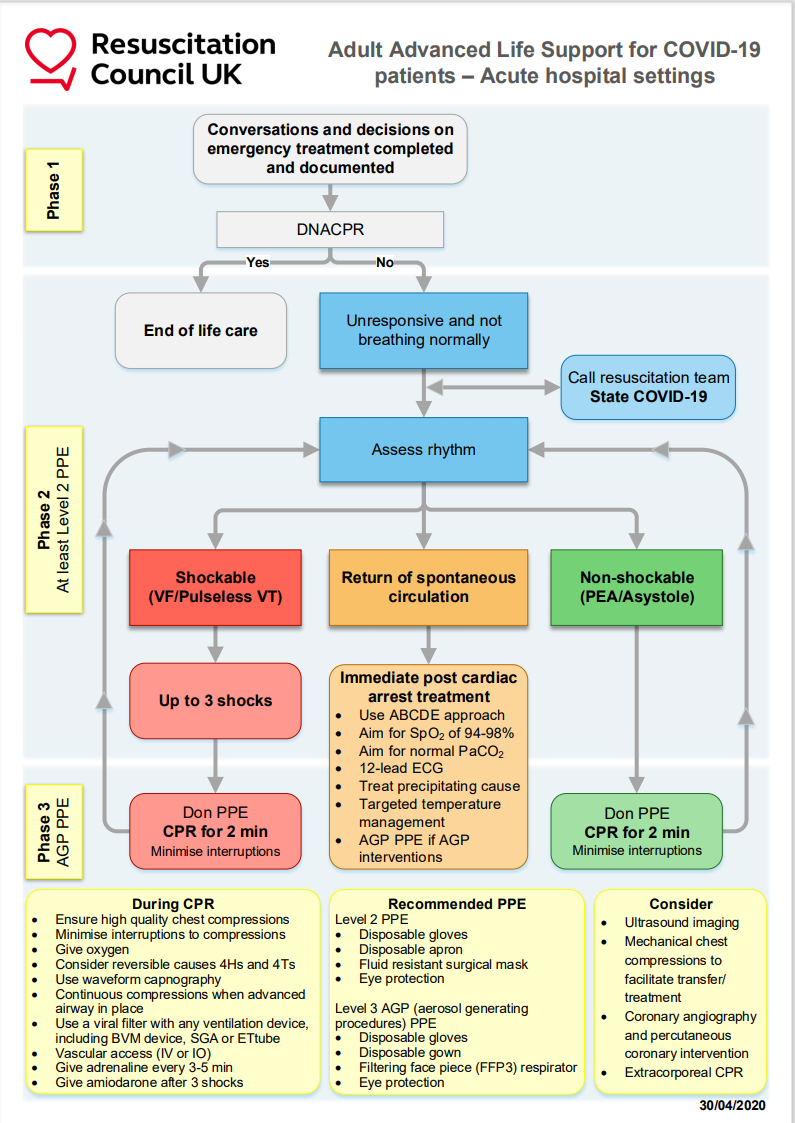
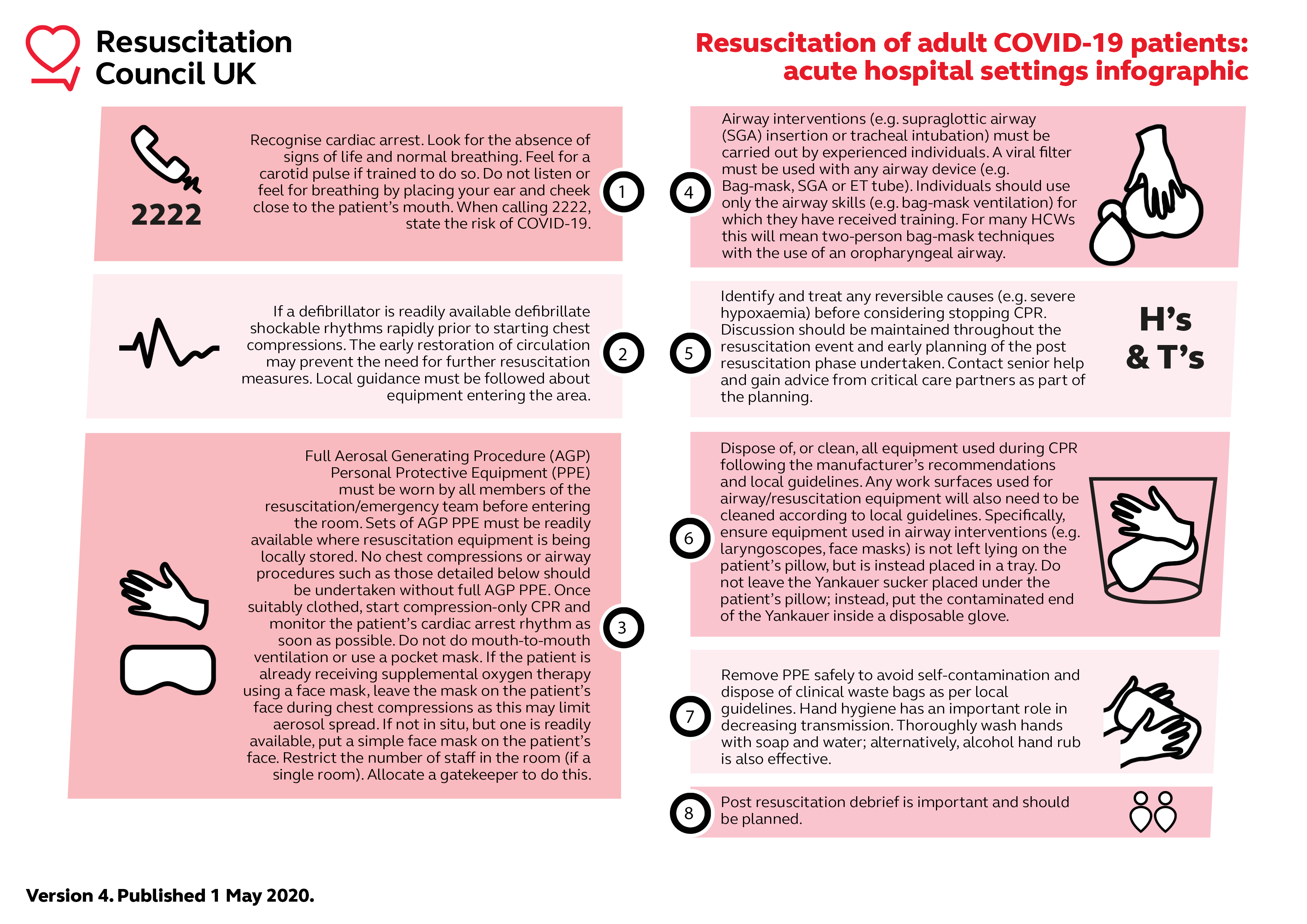
📸 Resuscitation Algorithms / Images
Replace older COVID-specific images with the current local or Resuscitation Council UK adult ALS algorithm where possible.
💡 Clinical Pearls
- Shockable arrest is primarily a defibrillation problem; do not delay shocks.
- Non-shockable arrest is primarily a reversible-cause problem; give early adrenaline and search actively.
- After any shock, restart CPR immediately without checking pulse or rhythm.
- Capnography helps confirm airway placement, monitor CPR quality and identify possible ROSC.
- Good ALS is team-based: leadership, closed-loop communication and anticipation prevent pauses.
📚 References
- Resuscitation Council UK: Adult Advanced Life Support Guidelines 2025
- Resuscitation Council UK: Adult ALS Algorithm 2025
- NICE CKS: Cardiac arrest — out-of-hospital care, advanced life support adult
Resuscitation - Advanced Life Support
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery