
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Endoscopic Retrograde Cholangiopancreatography (ERCP)
Related Subjects: |Upper Gastrointestinal Bleed |Oesophageal Variceal Bleeding |Dieulafoy Lesion |Mallory-Weiss Tear |Gastric Cancer |Peptic Ulcer Disease |Hypovolaemic or Haemorrhagic Shock |Carcinoma of the Gallbladder |Carcinoma of the Bile Duct |Cholangiocarcinoma
🧾 Magnetic Resonance Cholangiopancreatography (MRCP) is now the preferred diagnostic tool for suspected biliary obstruction. ⚡ Endoscopic Retrograde Cholangiopancreatography (ERCP) is reserved mainly for therapeutic interventions such as stone extraction, sphincterotomy, and stent placement.
📖 About ERCP
- Combines upper GI endoscopy with fluoroscopic X-ray imaging.
- Used to visualise the bile ducts, pancreatic duct, and gallbladder.
- Crucially, ERCP is both diagnostic and therapeutic (unlike MRCP).
🩺 ERCP Procedure
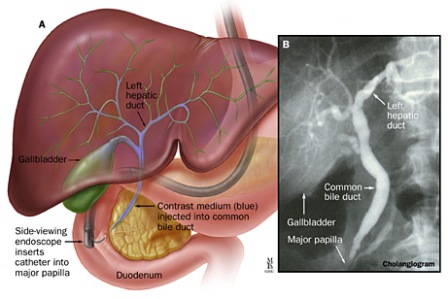
During ERCP, an endoscope is advanced to the duodenum. The bile duct is cannulated, and contrast dye is injected under X-ray guidance. ➡️ This provides detailed duct imaging and allows real-time interventions (stone removal, stent placement, biopsies).
📌 Indications for ERCP
- 🪨 Diagnosis and removal of common bile duct (CBD) stones.
- 🧬 Investigation and dilatation/stenting of biliary strictures (benign or malignant).
- 🧠 Diagnosis and palliation in cholangiocarcinoma or pancreatic cancer.
- ✂️ Sphincterotomy – cutting the sphincter of Oddi to aid stone clearance.
- 🩺 Pancreatic duct stenting in selected cases.
- 🔬 Biopsy or brush cytology of strictures or tumours.
🔎 Procedure Steps
- 🔒 Patient fasts and receives IV sedation ± analgesia.
- 📍 Endoscope passed via mouth → stomach → duodenum.
- 💉 Cannulation of bile/pancreatic duct, followed by contrast injection.
- 🧾 X-rays taken to identify stones, strictures, or tumours.
- ⚙️ Interventions performed as required (stone extraction, stenting, biopsy, sphincterotomy).
🪨 Example: Large CBD Stone
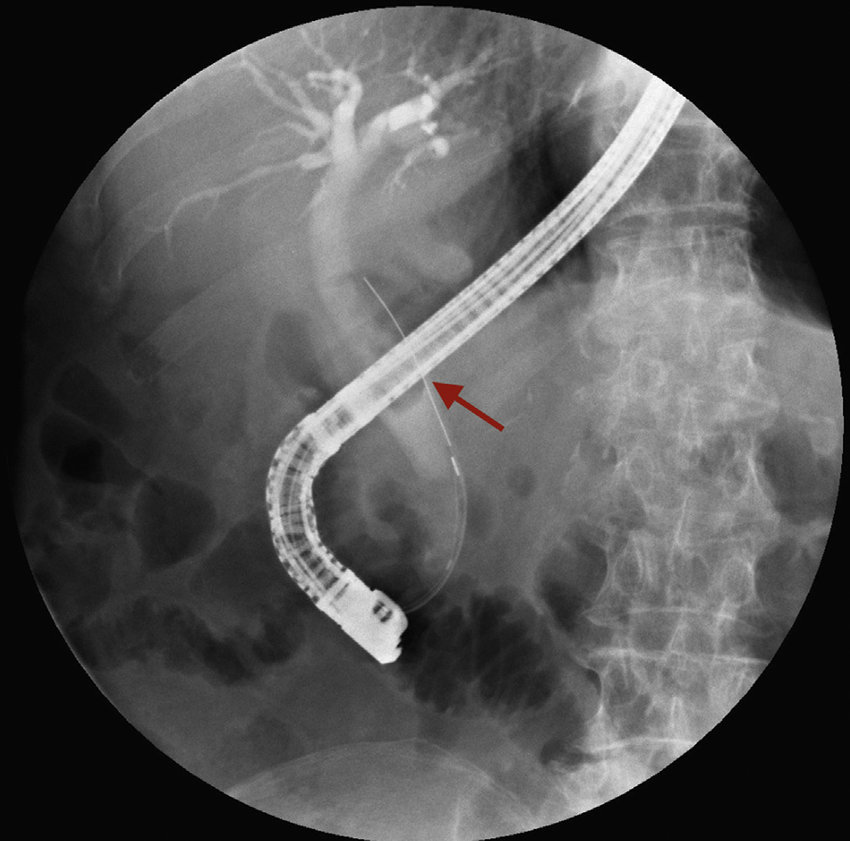
ERCP allows direct removal of obstructing CBD stones, restoring bile flow and preventing jaundice or cholangitis.
⏱️ Duration
- Typically lasts 60–120 minutes.
- Patients are sedated; recovery requires monitoring for a few hours post-procedure.
📝 Pre-Procedure Checklist
- ✅ Clotting screen (INR, platelets) if sphincterotomy likely.
- ✅ Review anticoagulants/antiplatelets → liaise with gastroenterology/haematology if on warfarin or DOACs.
- ✅ Consent discussion: include risk of pancreatitis, bleeding, infection, perforation.
⚠️ Potential Complications
- 💤 Sedation-related respiratory compromise.
- 🩸 Bleeding (~2% risk, especially post-sphincterotomy).
- ⚡ Acute pancreatitis (~5% risk; most common serious complication).
- 🦠 Cholangitis (biliary infection).
- 🕳️ Perforation of duodenum or ducts.
- ☢️ Cumulative radiation exposure (rarely significant).
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery