
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Hodgkin Lymphoma ✅
Related Subjects: |Hodgkin Lymphoma |Non Hodgkin Lymphoma |Diffuse large B-cell lymphoma |Intravascular large B-cell lymphoma |Mantle cell lymphoma |Marginal Zone Lymphoma |Gastric (MALT) Lymphoma |Primary CNS Lymphoma (PCNSL) |Burkitt's lymphoma |Follicular Lymphoma |Hodgkin vs Non-Hodgkin Lymphoma |Myeloproliferative disorders
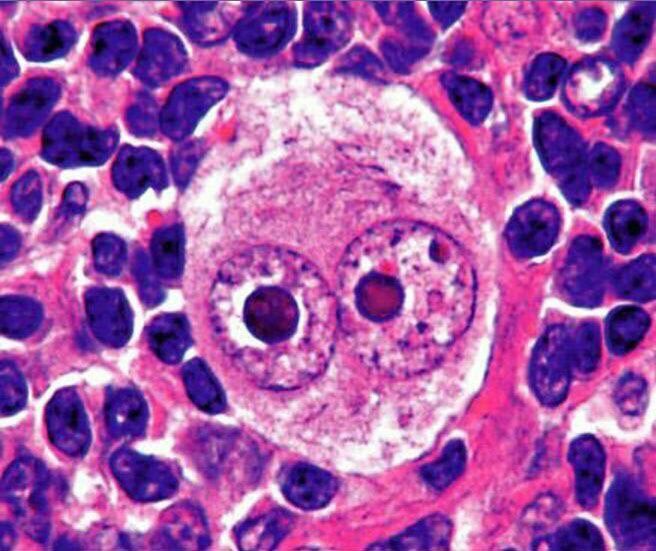
🩸 Hodgkin lymphoma (HL) is a malignant lymphoma characterised by Reed–Sternberg cells within an inflammatory background. It is one of the most curable cancers in modern haematology, especially when diagnosed early and treated appropriately.
✅ UK guidance framing: in primary care, the priority is early recognition and urgent referral. In adults with unexplained lymphadenopathy, especially with fever, drenching night sweats, weight loss, pruritus, or shortness of breath, think lymphoma and refer on a suspected cancer pathway.
📖 About
- Hodgkin lymphoma is a cancer of B-lymphocyte lineage.
- It usually arises in lymph nodes and often spreads in a relatively contiguous nodal pattern.
- It is much less common than non-Hodgkin lymphoma.
- It is highly treatable, and many patients are cured.
📊 Epidemiology
- There are around 2,000 new cases per year in the UK.
- HL accounts for roughly 10% of lymphomas in the UK.
- It has a bimodal age distribution, with one peak in younger adults and another in older adults.
- Incidence and mortality are slightly higher in men.
🧬 Pathophysiology & Aetiology
- HL arises from abnormal germinal-centre/post-germinal-centre B cells.
- The malignant Reed–Sternberg cells are few in number, but they release cytokines and chemokines that recruit a dense inflammatory infiltrate.
- This inflammatory microenvironment explains many systemic symptoms, including fever, weight loss, night sweats, pruritus, and raised ESR.
- EBV is associated with a proportion of cases, particularly in mixed cellularity disease and in immunosuppressed patients.
⚠️ Risk Factors
- 👶 Age: most common in younger adults, with a second later-life peak.
- ♂️ Sex: slightly more common in men overall.
- 👨👩👧 Family history: modestly increases risk.
- 🦠 EBV infection: associated with some cases.
- 🛡️ Immunodeficiency: including HIV and post-transplant immunosuppression.
🔬 Histological Subtypes
- Classical Hodgkin lymphoma:
- Nodular sclerosis: most common; often affects young adults and commonly involves the mediastinum.
- Mixed cellularity: more often linked with EBV and immunosuppression.
- Lymphocyte-rich: less common; generally favourable prognosis.
- Lymphocyte-depleted: rare and more aggressive.
- Nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL) is a distinct entity and behaves differently from classical HL.
📍 Staging (Ann Arbor)
| Stage | Description |
|---|---|
| I | Single lymph node region or single extralymphatic site |
| II | 2 or more nodal regions on the same side of the diaphragm |
| III | Nodal disease on both sides of the diaphragm, possibly with splenic involvement |
| IV | Diffuse/disseminated extranodal involvement (for example marrow, liver, lung) |
| A | No B symptoms |
| B | B symptoms present |
🔥 B Symptoms
- 🌡️ Fever
- 😰 Drenching night sweats
- ⚖️ Unexplained weight loss of more than 10%
- These reflect a systemic inflammatory response and have staging/prognostic significance.
🧑⚕️ Clinical Features
- Painless lymphadenopathy is the commonest presenting feature.
- Nodes are often firm, rubbery, and non-tender.
- Common sites: cervical, supraclavicular, mediastinal, and axillary nodes.
- General symptoms: fatigue, fever, night sweats, weight loss.
- Pruritus can occur and may precede diagnosis.
- Mediastinal disease may cause cough, chest discomfort, or breathlessness.
- Alcohol-related node pain is a rare but classic association.
- Splenomegaly may be present.
🧪 Investigations
- Blood tests: FBC, U&E, LFTs, ESR, CRP, LDH, urate, and baseline virology as guided by treatment planning.
- Excisional lymph node biopsy is the preferred diagnostic test.
- Histology typically shows Reed–Sternberg cells; classical HL is often CD15+ and CD30+.
- PET-CT is central to staging and response assessment in modern HL practice.
- CT may also be used for anatomical staging.
- Bone marrow biopsy is now selective rather than routine in all patients.
- Baseline echocardiogram or equivalent cardiac assessment is important if anthracyclines are planned; pulmonary assessment may be needed if bleomycin is being considered.
💊 Management
- Management is specialist-led and depends on stage, bulk of disease, symptoms, age, comorbidity, and fitness.
- Early-stage disease is often treated with short-course combination chemotherapy ± involved-site radiotherapy.
- Advanced disease is usually treated with systemic combination chemotherapy, with radiotherapy reserved for selected bulky or residual sites.
- Relapsed or refractory disease may be treated with salvage chemotherapy, autologous stem cell transplant, and/or newer agents such as brentuximab vedotin or PD-1 inhibitors.
- Supportive care includes fertility counselling, infection risk management, and treatment-toxicity monitoring.
💉 Treatment Pearls
- ABVD has been a longstanding backbone regimen in classical HL.
- Doxorubicin can cause cardiotoxicity; bleomycin can cause pulmonary toxicity.
- Older or frailer patients often need modified treatment because toxicity can outweigh benefit.
- Modern management increasingly uses response-adapted PET-guided strategies.
🩺 NICE/UK Primary Care Pearl
Think of Hodgkin lymphoma in any adult with unexplained lymphadenopathy, especially if there is fever, drenching night sweats, weight loss, pruritus, or shortness of breath. Normal initial blood tests do not exclude lymphoma.
📚 References
- NICE NG12: Suspected cancer: recognition and referral
- NICE CKS: Haematological cancers - recognition and referral
- British Society for Haematology: First-line management of classical Hodgkin lymphoma
- Cancer Research UK: Hodgkin lymphoma statistics
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery