
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
AIDS HIV Infection and a Fever ✅
Related Subjects: |AIDS (HIV) Neurological Disease |AIDS (HIV) Respiratory disease |AIDS Dementia Complex (HIV) |AIDS HIV Infection |AIDS(HIV) Gastrointestinal Disease |Acute Retroviral Syndrome (HIV) |HIV and Post-Exposure Prophylaxis (PEP) |HIV and Pre-exposure prophylaxis |HIV associated nephropathy (HIVAN) |HIV disease Assessment |Immune Reconstitution Syndrome |AIDS HAART Antiretrovirals |Kaposi sarcoma (KS)
| Algorithm - Approach to Fever in an HIV Patient (by CD4 Count) 🧪🌡️ |
|---|
|
Teaching Commentary 📘
Anchor your thinking in the CD4 count: - <200 → PCP, candidiasis - <100 → toxoplasmosis, cryptococcus - <50 → CMV, MAC. Remember “common things are common” - bacterial pneumonia, sepsis still predominate in the UK. Early ART reduces severe OIs, but knowledge of CD4 thresholds is essential for exams. 🌡️ Many patients with HIV may be asymptomatic. Always consider risk factors, recent exposures, and perform early testing.
📌 Introduction 🧬
- HIV prognosis has dramatically improved with HAART.
- Late diagnosis (low CD4) worsens outcomes.
- Current common causes of death: CAD, liver failure (HBV/HCV), lymphoma.
- HIV is now a chronic manageable disease with near-normal life expectancy if treated early.
🦠 Virus Overview
- HIV-1: Globally predominant, more virulent.
- HIV-2: Less virulent, mainly West Africa, resistant to NNRTIs.
🔬 Structure & Viral Cycle
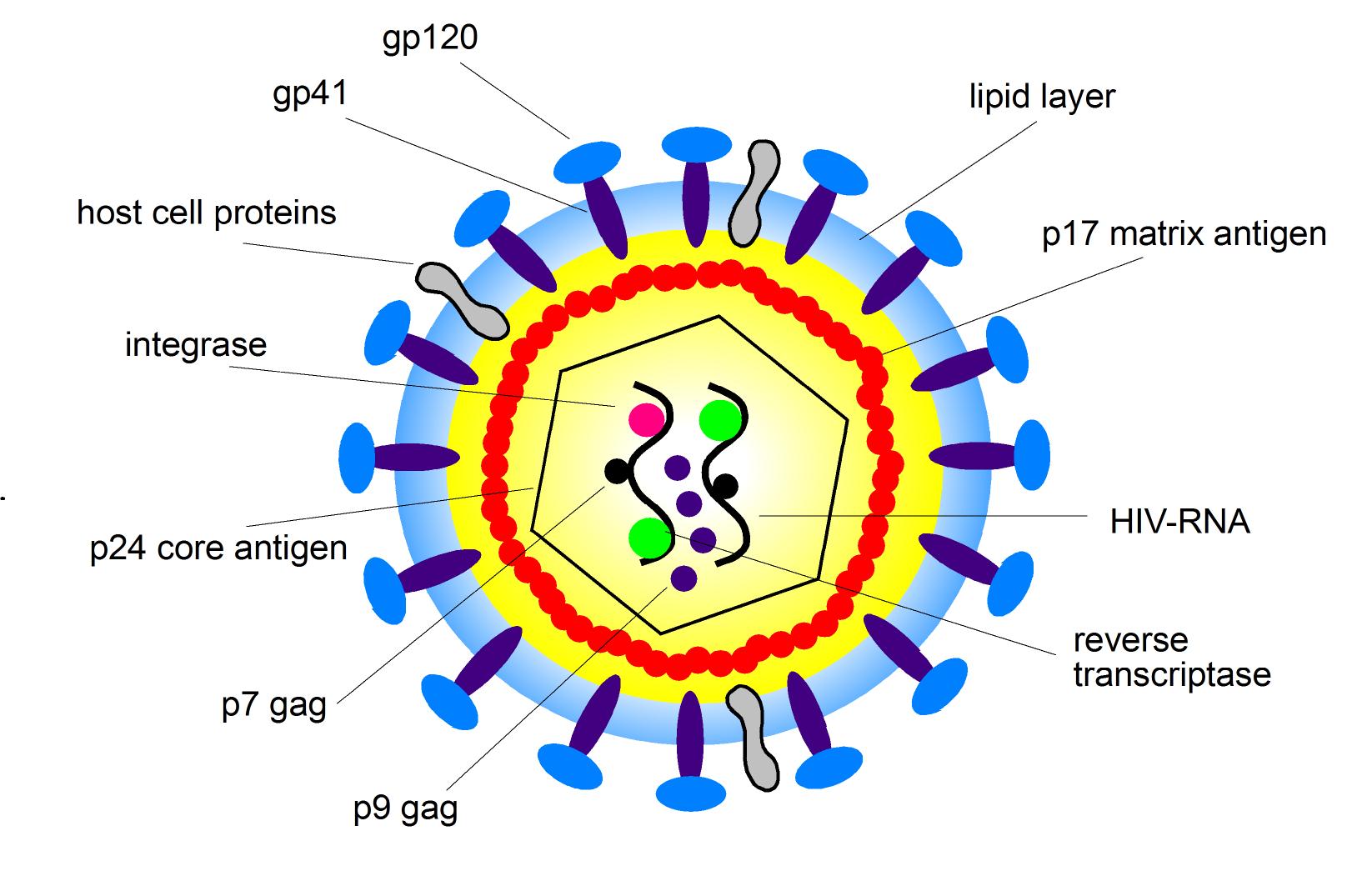
- Single-stranded RNA retrovirus (lentivirus)
- gp120: binds CD4 + CCR5/CXCR4 → entry
- gp41: fusion protein
- p24 capsid antigen: diagnostic marker
- Reverse transcriptase, integrase, protease: essential enzymes
🌀 Viral Life Cycle
- gp120 binds CD4 → chemokine receptor (CCR5/CXCR4)
- Fusion via gp41 and entry into cell
- Reverse transcription: RNA → DNA
- Integration into host genome via integrase
- Viral proteins synthesized by host machinery
- Virion assembly and release
🧬 Genes & Tropism
- gag = structural proteins; pol = enzymes; env = envelope (gp120, gp41)
- tat, rev = regulatory proteins; vif, vpr, vpu = accessory proteins
- Targets: CD4+ T cells, macrophages, dendritic cells → gradual CD4 depletion → immunodeficiency
📡 Transmission & Epidemiology
- Sexual contact (↑ risk with STIs) 💏
- Blood: needles, transfusions 💉
- Vertical: pregnancy, delivery, breastfeeding 🤱
- Worldwide burden highest in Sub-Saharan Africa 🌍
- Window period: 2–6 weeks → antibody-negative but highly infectious ⚠️
🔎 Clinical Clues to Test HIV
- Herpes zoster, recurrent infections
- Unexplained lymphadenopathy, fever
- Recurrent pneumonia, TB, lymphoma
⚠️ AIDS-Defining Conditions
- Infections: PCP, cryptococcosis, CMV, TB, MAC
- Cancers: Kaposi’s sarcoma, invasive cervical cancer, NHL
- Other: HIV encephalopathy, wasting syndrome
💊 ART & Prophylaxis
- Start ART for all patients, irrespective of CD4
- Suppress viral load, restore CD4, prevent transmission
- Prophylaxis:
- CD4 <200 → co-trimoxazole for PCP
- CD4 <100 → fluconazole for cryptococcus (high-risk)
- CD4 <50 → azithromycin/clarithromycin for MAC, regular fundoscopy for CMV
- Monitor: viral load, CD4, renal, liver, metabolic profile
- Vaccinations: inactivated vaccines; live vaccines avoided if CD4 <200
CD4 Count Thresholds & Opportunistic Infections 📊
| CD4 Count | Common Opportunistic Infections 🦠 | Prophylaxis / Notes 💊 |
|---|---|---|
| <500 | Oral candidiasis, shingles, Kaposi’s sarcoma | No routine prophylaxis; start ART |
| <200 | PCP, oesophageal candidiasis, cryptosporidium | Co-trimoxazole daily (stop once CD4 >200 on ART) |
| <100 | Toxoplasmosis, cryptococcal meningitis, disseminated Candida | Co-trimoxazole for toxoplasmosis; consider fluconazole prophylaxis |
| <50 | CMV retinitis/colitis, MAC, PML | Azithromycin weekly for MAC; regular fundoscopy for CMV monitoring |
📚 References
- NICE Guideline NG60: HIV testing and management
- BHIVA Guidelines
- Gazzard BG, HIV Medicine, 2018
- Panel on Opportunistic Infections in HIV-Infected Adults and Adolescents, CDC
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery