
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Acute Cardiogenic Pulmonary Oedema (CPO/LVF) ❤️
Related Subjects: |Heart Failure with preserved and reduced EF |Heart Failure and Pulmonary Oedema |Loop Diuretics |Entresto Sacubitril with Valsartan |Ivabradine |Furosemide |Angiotensin Converting Enzyme Inhibitors |Cardiac Resynchronisation Therapy (CRT) Pacemaker
💔 Cardiogenic Pulmonary Oedema (CPO) is a medical emergency. Often triggered by STEMI, arrhythmia, or mechanical failure. Always exclude these early. A simple bedside echo is invaluable. Acute pulmonary oedema is usually driven by a sudden rise in left-sided filling pressures (LV failure/acute MR/MI, hypertensive crisis), forcing fluid across the alveolar-capillary membrane. Your early wins are: improve oxygenation/ventilation (CPAP), offload the lungs (diuresis), and reduce preload/afterload (vasodilators) while treating the trigger.
| 💔 Emergency Management: Cardiogenic Pulmonary Oedema (CPO) |
|---|
|
🪑 Position → Sit upright, comfort, legs dependent, reassure, may need catheter
🫁 Oxygen → Maintain sats >92% (88–92% if COPD); CPAP if hypoxic 💧 Diuretics → Furosemide 40–80 mg IV bolus often as 4mg/kg. Diuresis and venodilates 💉 Opiates → Morphine 2.5–5 mg IV slow + antiemetic 💊 Nitrates → GTN spray; IV infusion if SBP >110 mmHg 🫀 Arrhythmias/STEMI → Treat Fast AF (Digoxin, Amiodarone) /VT (Amiodarone or DC shock), urgent PCI if STEMI 🔌 Advanced Support → CPAP 5–10 cmH₂O/NIV, balloon pump, dialysis if needed, Papillary rupture / VSD → balloon pump + urgent surgery |
💡 Mnemonic: sit up and FONAM = Furosemide, Oxygen Nitrates Arrhythmia Morphine,
📖 About
- CPO = acute left ventricular dysfunction → pulmonary venous hypertension → alveolar flooding.
- Rapidly leads to respiratory failure ± cardiogenic shock.
- 30-day mortality ~15% if NT-proBNP >5000 ng/L.
- LV systolic function strongly influences prognosis.
⚖️ Pathophysiology
- Normally: Plasma oncotic pressure (~25 mmHg) holds water in; Pulmonary capillary pressure (~7–12 mmHg) pushes fluid out.
- If PCP > POP → alveolar oedema → hypoxia, ↑ work of breathing.
🔎 Aetiology
- Poor systolic function (e.g. MI).
- Poor diastolic function (HFpEF).
- Valve lesions (MR, AR, AS).
- Arrhythmias (AF, VT, bradycardia).
- Hypertension, myocarditis, cardiomyopathy.
- Fluid overload (blood transfusion, renal failure).
❓ Precipitating Causes
| Cause | Clues | Diagnostics |
|---|---|---|
| MI | Chest pain, diaphoresis | ECG, troponin, echo |
| AF | Palpitations, irregular pulse | ECG, echo |
| HTN | Headache, chest pain | BP, LVH on echo |
| Valvular disease | Murmur, dyspnoea | Echo, Doppler |
| PE | Pleuritic pain, haemoptysis | CTPA, D-dimer |
| Sepsis | Fever, hypotension | Blood cultures, lactate |
| Drug/alcohol | Recent change | Medication review |
📊 Clinical: Left vs Right HF
The patient may be grey cold clammy and dramatically breathless and struggling to breath with a tachycardia and S3 and possibly murmurs, there is a raised JVP and lungs have fine inspiratory crackles. The sats may be low. Urgent management is needed.
- Left-sided: Tachypnoea, Tachycardia, S3, Murmurs, Orthopnoea, PND, bibasal creps, “bat-wing” CXR.
- Right-sided: Raised JVP, hepatomegaly, ascites, oedema.
- Often coexist → congestive HF.
🧪 Investigations (Acute Cardiogenic Pulmonary Oedema)
- Bedside (immediate):
- Vitals + monitoring: RR, BP, HR, temperature, continuous SpO2 + ECG monitoring.
- ECG (12-lead): look for ACS (ST/T changes), arrhythmia (AF, VT), LVH/strain, conduction disease.
- ABG/VBG: pO2/pCO2, pH, HCO3−; identify hypercapnia/tiring (important for NIV/ITU decisions).
- Lactate: marker of hypoperfusion/shock and severity.
- Glucose: especially if diabetic/altered mental state.
- Urine output: catheter if severe illness; helps gauge diuretic response and perfusion.
- Bloods:
- FBC: anaemia (reduces oxygen delivery), leukocytosis (infection trigger).
- U&E/creatinine: baseline renal function, K+/Na+ before diuresis/ACEi; guides dosing and safety.
- LFTs: hepatic congestion or hypoperfusion (“shock liver”).
- Troponin: MI/ischemia trigger (interpret in context; may be type 2 rise in severe HF).
- NT-proBNP: supports HF diagnosis if uncertain (less helpful if obvious clinically or known HF).
- CRP: if infection suspected; blood cultures before antibiotics if septic.
- TFTs: not urgent in resus, but useful if AF/new HF or unexplained decompensation.
- Mg/Ca/phosphate: if arrhythmia or on diuretics (electrolytes drive ectopy and rate control success).
- Imaging:
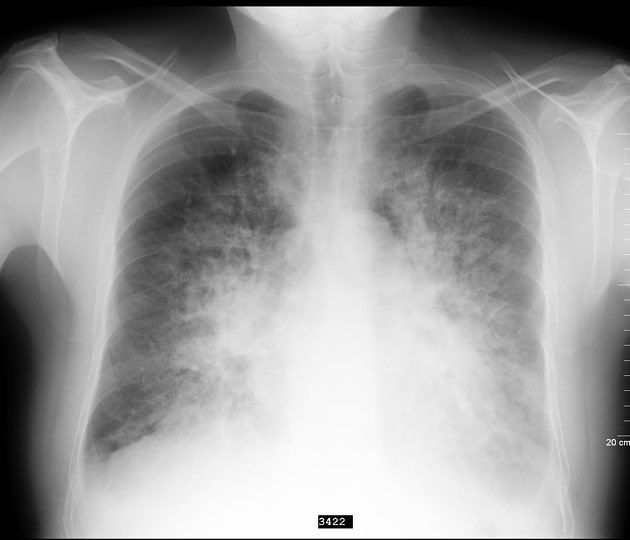
- CXR: cardiomegaly, upper lobe diversion, interstitial oedema (Kerley B lines), perihilar “bat-wing” shadowing, pleural effusions; also exclude pneumonia/pneumothorax.
- Point-of-care ultrasound (if available): lung B-lines, pleural effusions, IVC size; rapid bedside support for congestion.
- Echocardiography (urgent if severe/unclear): LV/RV function, regional wall motion (ischaemia), valve lesions (acute MR/AS), pericardial effusion/tamponade, pulmonary pressures.
- Advanced / specialist tests (selected cases, not acute resus):
- CT pulmonary angiography: if PE is a realistic alternative/trigger (especially if disproportionate hypoxia, RV strain).
- Coronary angiography: if STEMI/NSTEMI or ongoing ischaemia driving ACPO (cardiology pathway).
- Cardiac MRI: myocarditis/infiltrative disease/scar assessment once stabilised.
- Nuclear imaging (SPECT/PET): viability/ischaemia assessment in chronic planning rather than acute management.
⚡ Complications
- Respiratory failure:
- Type 1 (hypoxaemic): alveolar flooding + V/Q mismatch → low pO2.
- Progression to Type 2 (hypercapnic): fatigue, reduced minute ventilation, worsening alveolar ventilation (red flag for NIV failure/ITU).
- Cardiac complications:
- Arrhythmias: AF with fast rate (worsens filling), VT/VF, bradyarrhythmias; risk of sudden cardiac death.
- Myocardial ischaemia/infarction: ACPO can be both a cause and consequence of ACS (type 1 vs demand-mediated injury).
- Cardiogenic shock: “cold + wet” phenotype with hypoperfusion, rising lactate, oliguria.
- Renal dysfunction:
- AKI / cardiorenal syndrome: low forward flow + venous congestion + diuretics/ACEi exposure → creatinine rise and diuretic resistance.
- Hepatic and splanchnic congestion:
- Congestive hepatopathy: cholestatic LFT pattern; can progress to marked transaminitis if hypoperfusion (“shock liver”).
- Gut oedema: impaired drug absorption (e.g., oral diuretics) and malnutrition.
- Electrolyte and acid–base problems:
- Hyponatraemia: dilutional (ADH-driven) and a marker of severe HF; worsens confusion/falls risk.
- Hypokalaemia / hypomagnesaemia: diuretics → ectopy/VT risk and digoxin toxicity risk.
- Hyperkalaemia: renal impairment + RAAS blockade; conduction disturbance risk.
- Metabolic alkalosis: aggressive diuresis; may worsen CO2 retention in vulnerable patients.
- Thromboembolism:
- VTE: immobility, inflammation and haemoconcentration; consider prophylaxis if safe.
- Stroke/systemic embolism: especially if AF or severe LV dysfunction with thrombus.
- Functional decline and vulnerability:
- Delirium: hypoxia, infection, metabolic disturbance, opioids.
- Frailty, sarcopenia/cachexia: chronic catabolism + inflammation; strongly predicts readmission and mortality.
- Pressure injury/falls: immobility, hypotension, polypharmacy.
💊 Management
- Call for help + monitor: Sit upright, continuous ECG, BP, SpO2, RR; IV access; strict fluid balance + urine output (catheter if very unwell).
- Immediate investigations: ABG/VBG (± lactate), U&E/creatinine, FBC, troponin, glucose; CXR; ECG; bedside echo if available (LV function, MR, tamponade, RV strain).
- Oxygen strategy:
- Give O2 only if hypoxic. Aim SpO2 94–98% (or 88–92% if known CO2 retention).
- Early CPAP/NIV if severe distress/hypoxia despite O2 (often rapidly reduces work of breathing and improves gas exchange).
- Escalate to CCU/ICU/anaesthetics early if tiring, reduced consciousness, or NIV failing.
- Diuretics (decongestion):
- IV loop diuretic (e.g., furosemide 40 mg, 50 mg or 80 mg are all fine as needed or bumetanide 1-2 mg).
- Use higher doses if already on regular diuretics.
- Reassess response (symptoms, RR, crackles, urine output) and check renal function/electrolytes; consider infusion if poor response.
- Vasodilators (reduce preload/afterload):
- If SBP ≥ 110 mmHg and ongoing distress, consider GTN (sublingual or IV infusion) to rapidly reduce pulmonary capillary pressure.
- Avoid if hypotensive, severe aortic stenosis, or suspected RV infarct.
- Analgesia/anxiolysis:
- Avoid routine morphine; if used, do so cautiously (risk of respiratory depression/hypotension) and treat nausea.
- If shock/poor perfusion (cold + wet):
- Urgent senior/ICU input; consider inotropes/vasopressors (e.g., dobutamine ± noradrenaline) guided by echo/BP/perfusion.
- Look hard for reversible causes: MI, acute MR, arrhythmia, tamponade, massive PE.
- Treat the trigger (do not miss):
- ACS/MI: follow local ACS pathway; early cardiology review and reperfusion if indicated.
- Hypertensive ACPO: nitrates + CPAP are often key.
- Arrhythmia (AF with fast rate, VT): rate/rhythm control; urgent DC cardioversion if unstable.
- Acute valvular disease (e.g., acute MR): urgent echo + cardiothoracic/cardiology input.
- Fluid overload/renal failure: consider ultrafiltration/dialysis discussion if diuretic-resistant.
- When improving (transition to chronic HF care):
- Start/optimise disease-modifying therapy once stable: ACEi/ARB/ARNI, beta-blocker, MRA, and consider SGLT2 inhibitor where appropriate (per local/NICE guidance).
- Plan follow-up, education (daily weights, salt/fluids), and review precipitant + adherence.
- Advanced/definitive options (selected patients): CRT, ICD, LVAD, transplant (specialist pathways).
✅ Quick practical timing prompts
- 0–10 minutes: Sit up, monitoring, ABG/VBG, CPAP/NIV early if needed; if SBP ≥110, start GTN (SL then IV).
- 10–60 minutes: IV loop diuretic if congested; reassess BP/respiratory effort every 5–15 min; ECG/CXR; start ACS/arrhythmia pathway if indicated.
- 1–6 hours: Review urine output, repeat gases if severe, check U&E/K/Mg; consider escalation (infusions, inotropes, ICU) or specialist add-ons (metolazone/ultrafiltration) if resistant.
💊 Drug Table
| Drug | When to use | Typical dose | Timing / titration | Key cautions |
|---|---|---|---|---|
| GTN (glyceryl trinitrate) – sublingual spray/tablet | Severe dyspnoea with SBP ≥110 mmHg, especially hypertensive ACPO, while preparing IV infusion | 400 micrograms (1 spray) SL | Repeat every 5 minutes as needed while monitoring BP (commonly up to 3 doses) | Avoid/very cautious in hypotension, severe aortic stenosis, suspected RV infarct, recent PDE5 inhibitors |
| GTN – IV infusion | Ongoing distress despite oxygen/NIV, hypertensive pulmonary oedema | Start 5–10 micrograms/min | Increase by 5–10 micrograms/min every 3–5 min to symptom relief/BP target (often 20–200 micrograms/min; higher in monitored/ICU settings) | Continuous BP monitoring; stop/reduce if SBP falls or headache/hypotension develops |
| Furosemide – IV bolus | Clinical fluid overload, raised JVP/oedema, or known HF with congestion | 40 mg IV (if diuretic-naïve). If already on loop diuretic: same as or up to 2× their usual total daily oral dose as IV equivalent (senior-led) | Assess urine output and symptoms at 30–60 min. Consider repeat dosing if inadequate response | Can worsen hypotension/AKI; check U&E, watch K/Mg; avoid “diuretic-first” if profoundly hypertensive distress where nitrates/NIV are the rapid wins |
| Bumetanide – IV bolus | Alternative loop diuretic (e.g., poor response to furosemide, significant gut oedema, or local preference) | 1 mg IV (roughly ≈ furosemide 40 mg) | Reassess at 30–60 min; repeat/step up guided by response | Same cautions as loop diuretics; electrolyte depletion |
| Loop diuretic infusion (e.g., furosemide) | Diuretic resistance or repeated boluses needed; ICU/CCU-style pathway | Common approach: loading bolus then 5–10 mg/hour (ranges vary) | Titrate every 1–2 hours to urine output/clinical congestion; close U&E monitoring | Requires careful monitoring; risk of AKI, ototoxicity at very high doses/rapid pushes; senior-led |
| Morphine – IV (NOT routine) | Only if severe distress/pain/anxiety persists despite NIV and haemodynamic stabilisation, and senior agrees | 1–2 mg IV slow, small aliquots | Reassess after 5–10 min; repeat cautiously if needed | Respiratory depression, hypotension, nausea/vomiting; avoid if drowsy/CO2 retaining/hypotensive |
| Antiemetic (e.g., ondansetron) | If opioid used or significant nausea/vomiting | 4 mg IV | Single dose; reassess | QT prolongation risk (check ECG if concerns) |
| Dobutamine – IV infusion | Cold + wet (hypoperfusion/shock) with low cardiac output, typically ICU/CCU after echo/senior review | Start 2.5 micrograms/kg/min | Titrate every 10–20 min (typical range 2.5–20 micrograms/kg/min) to perfusion/BP/urine output | Arrhythmias, tachycardia, myocardial ischaemia; needs monitoring and clear diagnosis |
| Noradrenaline (norepinephrine) – IV infusion | Hypotension/shock to maintain perfusion pressure (often alongside inotrope), ICU pathway | Common starting range 0.05 micrograms/kg/min (local protocols vary) | Titrate every 2–5 min to MAP/BP target | Extravasation risk; ideally central access; treat the cause (MI, MR, tamponade etc.) |
| Nitroprusside – IV infusion (specialist) | Refractory hypertensive ACPO with severe afterload problem (ICU/CCU only) | Start 0.3 micrograms/kg/min | Titrate every 3–5 min (typical max ~10 micrograms/kg/min short term) | Cyanide/thiocyanate toxicity risk, hypotension; requires invasive monitoring |
| ACE inhibitor (e.g., captopril – oral) (selected cases) | After initial stabilisation, persistent hypertension with HF once not in shock and no contraindications | 6.25 mg PO | Can repeat/uptitrate cautiously after 30–60 min with BP monitoring (senior-led) | Avoid in hypotension, AKI, hyperkalaemia, bilateral RAS, pregnancy; not a “first 10 minutes” drug |
⚡ Additional interventions
| Trigger / scenario | Drug(s) | Typical dose | Timing / titration | Key cautions / notes |
|---|---|---|---|---|
| Suspected ACS / MI | Aspirin | 300 mg PO (chewed) if not already taken | Give immediately once ACS suspected (per ACS pathway) | Contra: true aspirin allergy, active major bleeding |
| Suspected ACS / MI | P2Y12 inhibitor (specialist pathway) | Common UK practice: Ticagrelor 180 mg PO loading or Clopidogrel 300–600 mg PO loading (varies by STEMI/NSTEMI pathway) | As per local cardiology/PCI pathway (often after ECG confirmation and discussion) | Bleeding risk; avoid if urgent surgery likely; follow trust protocol |
| Suspected ACS / ongoing ischaemic pain | GTN (as per core table) | SL 400 micrograms q5 min PRN; IV start 5–10 micrograms/min | Titrate every 3–5 min to pain relief/BP | Avoid in hypotension, severe AS, RV infarct, recent PDE5 inhibitors |
| AF with fast ventricular response (haemodynamically stable) | Digoxin (rate control in HF) | 500 micrograms IV (or PO) then 250 micrograms at 6 hours and again at 12 hours (max 1.0–1.5 mg in 24 h depending on age/renal function) | Slower onset; reassess rate and symptoms over hours | Reduce dose in elderly/renal impairment; toxicity risk (arrhythmias, GI, confusion); check K/Mg |
| AF with fast rate (stable, BP ok) | Amiodarone (rhythm control / rate control alternative) | 300 mg IV over 20–60 min, then infusion 900 mg over 24 h | Use when appropriate (often senior-led/cardiology) | Hypotension/bradycardia; interacts with warfarin/digoxin; needs ECG monitoring |
| Unstable tachyarrhythmia (AF/VT with hypotension, ischaemia, pulmonary oedema) | DC cardioversion | Energy per ALS protocol (biphasic escalating) | Immediate | Not a drug, but the correct “dose” is electricity; involve resus/anaesthetics |
| VT / Electrical storm (with ACPO) | Amiodarone | 300 mg IV over 20–60 min (can repeat per ALS), then 900 mg/24 h | Early, alongside correction of K/Mg and ischaemia treatment | Consider magnesium; urgent cardiology/ICU for recurrent VT/VF |
| Torsades / hypomagnesaemia | Magnesium sulfate | 2 g IV (8 mmol) over 10–15 min | May repeat once if needed; then consider infusion per protocol | Monitor reflexes/respiration in renal failure; correct K as well |
| Hypertensive emergency driving ACPO | GTN IV (first-line add-on) | Start 5–10 micrograms/min, titrate rapidly | Increase every 3–5 min to symptom/BP response | Often the “fastest fix” with CPAP; avoid if severe AS/RV infarct/hypotension |
| Acute severe mitral regurgitation (papillary muscle dysfunction/rupture, endocarditis etc.) | Vasodilator (GTN) ± inotrope (dobutamine) | GTN as above; dobutamine start 2.5 micrograms/kg/min | Titrate GTN every 3–5 min; dobutamine every 10–20 min | Needs urgent echo + cardiology/cardiothoracic; may require mechanical support/urgent surgery |
| Suspected sepsis/pneumonia precipitant | Antibiotics (per local guideline) | Depends on source and severity | Give within 1 hour if sepsis suspected | Fluid resuscitation must be cautious in ACPO-senior review; use vasopressors if shock rather than large fluids |
| Thromboembolism risk / immobility | VTE prophylaxis (if no contraindication) | Example: Enoxaparin 40 mg SC OD (adjust for renal function/weight) | Once stable and bleeding risk assessed | Follow local VTE policy; avoid if active bleeding/very high risk |
| Fluid overload + renal failure / diuretic resistance | Metolazone (specialist add-on) | 2.5 mg PO | Often single dose, reassess over 6–12 h; may repeat cautiously (senior-led) | Profound diuresis/hypoNa/hypoK; close U&E monitoring; usually HF specialist decision |
| Persistent congestion despite loops | Chlorothiazide IV (less common UK) / thiazide-type add-on | Varies by local availability | Specialist/ICU pathway | Electrolyte depletion; monitor Na/K/Mg closely |
| After stabilisation: start disease-modifying HF therapy | ACEi/ARB/ARNI; beta-blocker; MRA; SGLT2 inhibitor | Start low (agent-specific) once euvolaemic and BP/renal function acceptable | Usually on the ward once off IV nitrates/inotropes and not in AKI | Not “resus drugs”; avoid initiating/up-titrating beta-blocker during acute decompensation/shock |
📉 Prognosis
- HF prognosis worse than many cancers.
- EF <35% = poor marker.
- NT-proBNP correlates with survival.
- Consider palliative care in end-stage disease.
📚 References
Cases - Acute Heart Failure & Pulmonary Oedema
- Case 1 - Hypertensive Emergency 💥: A 72-year-old man with untreated hypertension presents acutely breathless at night, unable to lie flat. Exam: BP 210/110, tachypnoea, widespread crackles, S3 gallop. CXR: bilateral perihilar “bat-wing” shadowing. Diagnosis: Acute pulmonary oedema triggered by hypertensive crisis. Acute Management: Sit upright, oxygen, IV furosemide, IV GTN infusion, morphine if distressed, strict BP control. Monitor U&Es and fluid balance.
- Case 2 - Acute MI Complication ❤️: A 64-year-old man presents with acute chest pain followed by severe dyspnoea. Exam: hypotension, crackles to mid-zones, raised JVP, cool peripheries. ECG: anterior STEMI. Echo: severe LV systolic dysfunction. Diagnosis: Acute cardiogenic pulmonary oedema secondary to MI. Acute Management: Sit upright, O₂, IV diuretics, cautious opioids; urgent PCI for MI; inotropes or mechanical support (IABP) if shock persists.
- Case 3 - Acute Decompensation in Chronic HF 🌀: A 78-year-old woman with known HFrEF (EF 30%) presents with sudden worsening breathlessness after a chest infection. Exam: tachypnoeic, bibasal crackles, elevated JVP, peripheral oedema. BNP elevated, CXR: pulmonary congestion. Diagnosis: Acute decompensated heart failure with pulmonary oedema, triggered by infection. Acute Management: Sit upright, O₂, IV furosemide; treat infection (antibiotics); optimise chronic therapy (ACEi, beta-blocker, spironolactone) once stable.
Teaching Commentary 🧠
Acute heart failure with pulmonary oedema is a medical emergency. - Pathophysiology: raised LV end-diastolic pressure → pulmonary venous congestion → alveolar fluid → hypoxia. - Precipitants: MI, arrhythmias, hypertensive crisis, infection, fluid overload, non-compliance. - Clinical: severe breathlessness, orthopnoea, crackles, frothy pink sputum, gallop rhythm. - Acute management (“PODMAN”): Position upright, Oxygen, Diuretics (IV loop), Morphine, Afterload reduction (nitrates), Non-invasive ventilation if hypoxic. Long-term: optimise HF therapy (ACEi/ARNI, beta-blockers, MRA, SGLT2 inhibitors); lifestyle and fluid restriction; device therapy (CRT, ICD) in select patients.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery