Acromegaly and Giantism ✅
Related Subjects:
|Male Infertility
|Prolactin
|Prolactinoma
|Sheehan's syndrome
|Acromegaly and Giantism
🧬 Key Point: Measure serum IGF-1 when acromegaly is suspected ✅.
Random GH levels are pulsatile and unreliable ❌, whereas IGF-1 reflects integrated GH secretion over time and correlates with disease activity.
📖 About
- 👨⚕️ Usually caused by a GH-secreting pituitary adenoma (somatotroph tumour)
- 📏 Gigantism: GH excess before epiphyseal fusion → linear growth
- 🧑 Acromegaly: GH excess after epiphyseal fusion → soft tissue & bony overgrowth
- ⏳ Insidious onset → diagnosis often delayed by years
🧪 Aetiology
- ⛏️ Pituitary somatotroph adenoma (≈95%, often macroadenomas at diagnosis)
- 🧬 Activating Gsα (GNAS) mutations → ↑ cAMP → autonomous GH secretion
- 🧠 Rare: ectopic GHRH/GH-secreting neuroendocrine tumours (pancreas, lung)
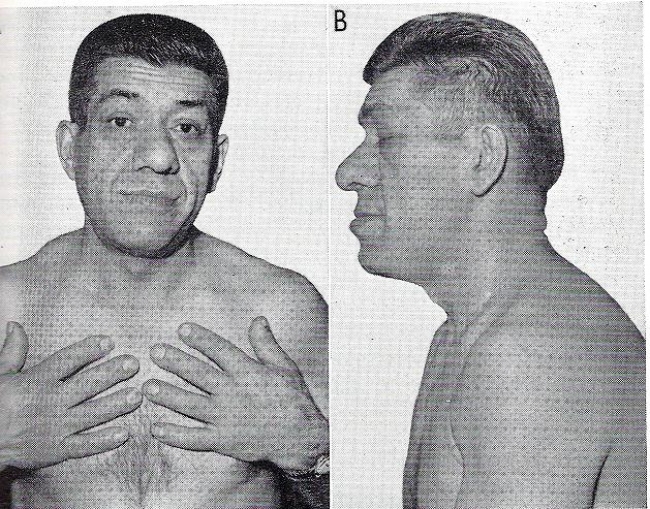
🩺 Clinical Features
- 📈 Cardiometabolic: hypertension, insulin resistance → T2DM
- 💦 Hyperhidrosis, seborrhoea, characteristic body odour
- 👃 Coarse facial features: enlarged nose, lips, tongue (macroglossia)
- 🦷 Interdental spacing, malocclusion
- 🖐 “Spade-like” hands, ring/shoe size ↑, thickened skin
- 🦴 Frontal bossing, supraorbital ridge prominence
- 😬 Prognathism (mandibular overgrowth)
- 🫀 Organomegaly: cardiomegaly (→ cardiomyopathy), hepatomegaly
- 🧠 Mass effect: headache, bitemporal hemianopia (optic chiasm compression)
- 💪 Proximal myopathy, fatigue
- 💫 Carpal tunnel syndrome (median nerve compression from soft tissue overgrowth)
- 📊 ↑ Risk of colorectal neoplasia (screening advised)
🤝 Associated Conditions
- 😴 Obstructive sleep apnoea (soft tissue airway narrowing)
- 💉 Type 2 diabetes mellitus
- 🦴 Osteoarthritis (cartilage overgrowth + joint stress)
- ❤️ Cardiomyopathy → leading cause of mortality if untreated
- 💦 Hyperhidrosis
- 📈 Hypertension
🔍 Investigations
- 🧪 Baseline bloods: FBC, U&Es, LFTs, glucose, HbA1c
- 📈 Screening test: ↑ serum IGF-1 (age-adjusted) → best initial test
- ✅ Diagnostic test: Oral glucose tolerance test (OGTT)
→ 75 g glucose should suppress GH to <0.4 µg/L (failure = acromegaly)
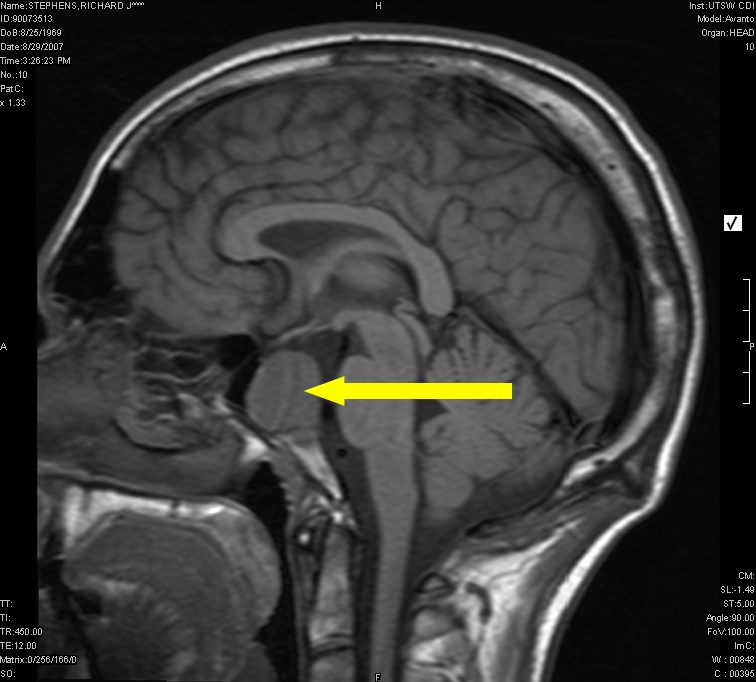
- 🧠 Pituitary MRI (with gadolinium) → identifies adenoma (macroadenoma common)
- 👁️ Formal visual field testing if suprasellar extension
- 🔄 Full pituitary profile: PRL, TFTs, cortisol, LH/FSH, sex hormones
- 📺 CT if MRI contraindicated
- 🔎 Colonoscopy (baseline ± surveillance)
- ❤️ ECG + echocardiogram → assess acromegalic cardiomyopathy
🧾 Differential Diagnosis
- GH-secreting pituitary adenoma
- Mixed GH/PRL adenoma
- Ectopic GHRH/GH secretion (neuroendocrine tumours)
- Severe insulin resistance syndromes (“pseudo-acromegaly”)
💊 Management
- 🎯 Treatment targets: Normal age-adjusted IGF-1 + GH <1.0 µg/L
- 🔪 First-line: Transsphenoidal surgery (potentially curative)
- ☢️ Radiotherapy: adjunct if residual disease (delayed effect; risk hypopituitarism)
- 💉 Medical therapy:
- Somatostatin analogues (octreotide, lanreotide) → ↓ GH secretion
- Dopamine agonists (cabergoline) → useful in mild disease or mixed tumours
- GH receptor antagonist (pegvisomant) → normalises IGF-1 (does not shrink tumour)
- 🧩 Hormone replacement for hypopituitarism (e.g. hydrocortisone, levothyroxine)
- 🔄 Follow-up: IGF-1 monitoring + periodic MRI (typically annually once stable)
📚 References