
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Parkinson disease
Related Subjects: Multiple System Atrophy (MSA) |Parkinson Plus syndromes |Parkinsonism |Idiopathic Parkinson disease |Acutely Ill Patient with Parkinson's disease |Progressive Supranuclear Palsy |Drug Induced Parkinson disease |Neuroleptic Malignant Syndrome |Parkinsonism–hyperpyrexia syndrome
🧠 Parkinson's Disease (PD) is a chronic, progressive neurological disorder affecting movement and non-motor functions. 👴 Most often seen in older adults, though genetic forms can present earlier.
ℹ️ About
- 🌀 Idiopathic PD: Tremor, rigidity, bradykinesia.
- 👵 More common in elderly, but younger onset with genetic variants.
🧬 Aetiology
- ⬇️ Dopaminergic neurons lost in the substantia nigra.
- ⚡ Disrupted communication in the basal ganglia.
- 🧩 Lewy bodies (α-synuclein inclusions) hallmark of PD pathology.
Pathology: Braak Staging
- 📈 Pathology spreads stepwise: brainstem → midbrain → cortex.
- 🚽 Early = constipation, REM sleep disorder; 🤲 Later = tremor, rigidity.
Genetics
- 🧬 PARK1 (α-synuclein): Early-onset, autosomal dominant.
- 🧬 PARK2 (parkin): Autosomal recessive, good response to L-Dopa.
🩺 Progressive Clinical Features
- ✋ Tremor: “Pill-rolling” resting tremor.
- 🐢 Bradykinesia: Slowness, difficulty initiating movement.
- 🪵 Rigidity: Limb stiffness, cogwheeling.
- ⚖️ Postural instability: Falls, poor balance.
- 🌙 Non-motor: depression, constipation, sleep disturbance, anosmia.
Stages of PD
- 1️⃣ Mild unilateral tremor.
- 2️⃣ Bilateral symptoms, slower movement.
- 3️⃣ Falls, significant motor difficulty.
- 4️⃣ Severe disability, daily assistance required.
- 5️⃣ Bedridden/wheelchair, hallucinations possible.
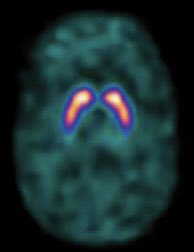
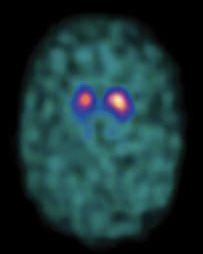
Diagnostic Imaging
- 🧲 MRI: Exclude mimics (vascular PD, NPH).
- 📊 DaT Scan: Differentiates PD from essential tremor.
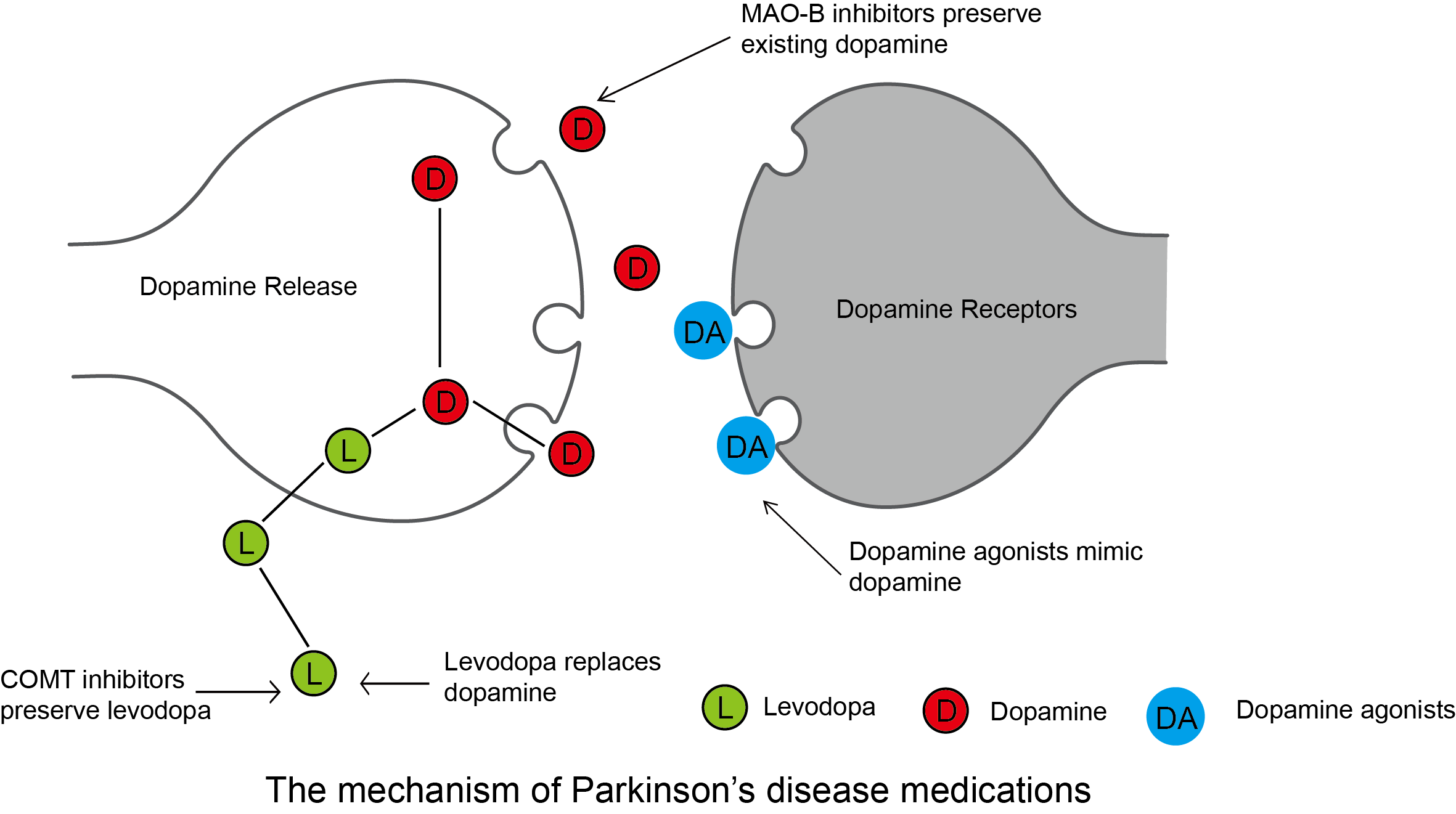
Pharmacological Management
- 💊 Levodopa + Carbidopa (Sinemet): Gold standard, best for motor symptoms.
- 🟤 COMT inhibitors: Prolong levodopa action (e.g. entacapone).
- 🟢 Dopamine agonists: Ropinirole, pramipexole (younger patients).
- 🔵 MAO-B inhibitors: Rasagiline, selegiline (mild disease).
- 🟣 Anticholinergics: Tremor-dominant PD (younger patients).
- 🟡 Amantadine: Useful for dyskinesias.
🧠 About Parkinson’s Drug Management
- Parkinson’s disease results from dopamine deficiency in the basal ganglia, leading to tremor, rigidity, bradykinesia, and postural instability.
- The main goal of therapy is to restore dopaminergic tone, reduce motor and non-motor symptoms, and improve quality of life.
- Treatment strategies are individualised based on patient age, disease stage, cognitive function, frailty, and comorbidities.
- Combination therapy is often required as the disease progresses, and management should be supervised by a specialist in movement disorders.
💊 Main Drug Classes & Dosing
- 1️⃣ Levodopa + DDC inhibitor (co-careldopa, co-beneldopa)
- Mechanism: Levodopa is converted to dopamine in the brain; carbidopa or benserazide blocks peripheral metabolism.
- First-line in patients >70 years or with cognitive impairment.
- Dose:
- Start low (e.g. co-careldopa 12.5/50 mg TDS) and titrate gradually.
- Typical maintenance: 50/200 mg TDS–QDS, adjusted to clinical response.
- Modified formulations:
- Rytary (IPX203): extended-release capsule for smoother “on” time.
- LCIG (Duopa/Duodopa): intestinal gel via pump for continuous delivery.
- Inhaled Levodopa (Inbrija): rescue option for sudden “off” episodes, onset within 10 minutes.
- ND0612: subcutaneous infusion for 24-hour steady levels (emerging therapy).
- ⚠️ Common side effects: dyskinesia, orthostatic hypotension, hallucinations, nausea, “on–off” fluctuations with long-term use.
- 2️⃣ Dopamine Agonists (pramipexole, ropinirole, rotigotine patch, apomorphine)
- Mechanism: Directly stimulate dopamine receptors (mainly D2/D3), bypassing presynaptic neurons.
- Use: Monotherapy in early PD for younger adults, or as add-on to levodopa in advanced disease.
- Examples & Doses:
- Pramipexole: 0.125 mg TDS → titrate to max 1.5 mg TDS.
- Ropinirole: 0.25 mg TDS → increase; XL forms available for once-daily dosing.
- Rotigotine patch: start 2 mg/24 h → titrate to max 16 mg/24 h.
- Apomorphine: subcutaneous rescue injection or continuous infusion (specialist use only).
- ⚠️ Side effects: impulse control disorders (gambling, hypersexuality), hallucinations, nausea, ankle oedema, sudden sleep attacks.
- Note: Start low, titrate slowly, monitor mood and sleep; avoid abrupt withdrawal to prevent dopamine agonist withdrawal syndrome.
- 3️⃣ MAO-B Inhibitors (selegiline, rasagiline, safinamide)
- Mechanism: Inhibit monoamine oxidase-B, decreasing dopamine breakdown in the brain.
- Use: Early PD (as monotherapy) or adjunct therapy to prolong levodopa effect and reduce “off” episodes.
- Dosing:
- Selegiline: 5 mg OD or BD.
- Rasagiline: 1 mg OD.
- Safinamide: 50 mg OD → may increase to 100 mg OD.
- ⚠️ Side effects: insomnia, headache, mild hallucinations; rare hypertensive crisis with tyramine-rich foods.
- Note: Avoid combining with serotonergic antidepressants or opioids due to serotonin syndrome risk.
- 4️⃣ COMT Inhibitors (entacapone, opicapone, tolcapone)
- Mechanism: Inhibit catechol-O-methyltransferase (COMT), prolonging levodopa’s half-life and “on” time.
- Use: Always as adjunct to levodopa when wearing-off occurs.
- Dosing:
- Entacapone: 200 mg with each levodopa dose (max 10/day).
- Opicapone: 50 mg once nightly (newer, long-acting).
- Tolcapone: 100–200 mg TDS; effective but limited by hepatotoxicity.
- ⚠️ Side effects: diarrhoea, urine discolouration (orange), dyskinesia, hepatotoxicity (tolcapone-monitor LFTs).
- 5️⃣ Amantadine
- Mechanism: NMDA receptor antagonist; enhances dopamine release and reduces reuptake.
- Dose: 100 mg OD–BD (max 300 mg/day); extended-release (Gocovri ER) once daily at bedtime.
- Use: Helps control levodopa-induced dyskinesias and provides mild symptomatic benefit.
- ⚠️ Side effects: hallucinations, livedo reticularis (mottled skin), ankle oedema, confusion, blurred vision.
- Note: Dose reduction required in renal impairment and elderly patients.
- 6️⃣ Anticholinergics (trihexyphenidyl, procyclidine)
- Mechanism: Block muscarinic receptors, restoring balance between dopamine and acetylcholine.
- Dose: Trihexyphenidyl 1 mg OD–BD (max 15 mg/day); adjust slowly.
- Use: Tremor-predominant PD in young, cognitively intact patients.
- ⚠️ Side effects: confusion, memory impairment, urinary retention, constipation, dry mouth - avoid in elderly.
- 7️⃣ Adjunct & Emerging Agents
- Adenosine A2A antagonist (Istradefylline): Adjunct to levodopa in patients with “off” episodes; reduces "off" time and improves mobility.
- GLP-1 receptor agonists (Exenatide, Lixisenatide): Under investigation for neuroprotective and disease-modifying benefits.
- Gene therapy (AADC vector, AXO-Lenti-PD): Experimental approaches to restore dopamine synthesis.
🧩 Key Points
- Levodopa remains the gold standard for symptomatic control.
- Long-acting and continuous delivery systems (LCIG, ND0612, Rotigotine patch) help minimize “off” time and fluctuation.
- Adjunct agents (MAO-B, COMT inhibitors, adenosine antagonists) prolong levodopa benefit.
- Tailor therapy to symptom pattern, lifestyle, and patient goals - avoid polypharmacy where possible.
- Monitor regularly for side effects such as dyskinesia, hallucinations, orthostatic hypotension, and impulse control disorders.
⚙️ Advanced / Rescue Therapies
- LCIG (Duopa/Duodopa): Continuous intrajejunal infusion for advanced PD with severe motor fluctuations.
- Apomorphine Pump: Delivers continuous dopamine agonist stimulation; used for complex “off” episodes.
- Inhaled Levodopa (Inbrija): Rapid rescue during sudden wearing-off; onset within 10 minutes.
- Deep Brain Stimulation (DBS): Non-pharmacologic option for selected patients unresponsive to medications.
✅ Summary
Parkinson’s disease management requires a stepwise, individualized approach. Start with levodopa-based therapy in older or cognitively impaired patients, and dopamine agonists or MAO-B inhibitors in younger individuals. Add COMT inhibitors or amantadine as the disease progresses to reduce fluctuations and dyskinesia. Advanced and long-acting formulations-both oral and infusion-based-are now enabling more stable motor control and improved quality of life. Levodopa remains the most effective treatment for Parkinson’s disease. Long-acting and continuous infusion forms improve symptom stability, while adjuncts-such as dopamine agonists, MAO-B inhibitors, and COMT inhibitors-help control motor fluctuations. Therapy should always be individualized to minimize side effects and optimize quality of life.
📋 NICE Simplified Pathway
- 👴 Older (>70) or cognitive impairment → Levodopa.
- 🧑 Younger (<70), no cognitive issues → Dopamine agonist or MAO-B inhibitor.
- ⚡ Escalate stepwise with COMT inhibitors, dopamine agonists, or amantadine if fluctuations develop.
- Specialist referral at all treatment stages.
🚑 Management When Unable to Swallow (NBM)
- 💧 Dispersible levodopa (Madopar® dispersible): can be given via NG tube.
- 🩹 Rotigotine patch: provides continuous dopaminergic stimulation.
- 💉 Apomorphine (SC injection/infusion): specialist initiation, useful for acute rescue.
- 📡 Duodopa® (levodopa–carbidopa intestinal gel): continuous PEG-J infusion.
- ⚠️ Never stop dopaminergic drugs suddenly → risk of Parkinsonism–Hyperpyrexia Syndrome.
⚠️ Key Cautions & Monitoring
- Impulse control disorders (gambling, hypersexuality, binge eating) with dopamine agonists.
- Hallucinations & psychosis with dopaminergic drugs.
- Postural hypotension with levodopa and dopamine agonists.
- Monitor LFTs with tolcapone.
- Adjust doses in renal impairment for amantadine.
Surgical
- 🧩 Deep Brain Stimulation (DBS): For advanced disease, subthalamic nucleus/globus pallidus targets.
Multidisciplinary Care
- 👩⚕️ Nurse specialist: medication timing, education.
- 🏃 Physiotherapy: balance, gait training.
- 🗣️ SLT: dysarthria, dysphagia.
- 🛠️ OT: adaptive aids, safety at home.
Hospital/Acute Considerations
- ⏰ Never delay PD meds (risk of severe deterioration, even NBM use NG or rotigotine patch).
- 🚫 Avoid antidopaminergic drugs (metoclopramide, haloperidol, prochlorperazine).
Non-Motor Complications
- 🚽 Constipation → macrogol, fluids, mobility.
- 📉 Orthostatic hypotension → fludrocortisone, midodrine.
- 🦠 Recurrent UTIs → hydration, constipation prevention.
- 👻 Psychosis/hallucinations → quetiapine, clozapine.
- 🧩 Dementia → rivastigmine (watch for tremor worsening).
Advance Care Planning
- 📝 Advance directives, lasting power of attorney.
- 🤝 Signposting to community support and respite care.
References
Cases - Parkinson’s Disease with Complications
- Case 1 - Motor Fluctuations (“Wearing Off”) ⏳: A 68-year-old man on levodopa for 7 years reports that tremor and rigidity return 3 hours after each dose. He experiences “on–off” fluctuations through the day. Complication: Motor fluctuations due to long-term levodopa use. Management: Shorten levodopa dosing intervals; add COMT inhibitor (entacapone) or dopamine agonist.
- Case 2 - Dyskinesias 💃: A 62-year-old woman develops involuntary writhing movements of her trunk and arms about 30 minutes after each levodopa dose. Complication: Levodopa-induced dyskinesia. Management: Lower levodopa dose; add amantadine; consider deep brain stimulation if severe.
- Case 3 - Parkinson’s Disease Dementia 🧠: A 75-year-old man with 10 years of PD develops progressive memory loss, visual hallucinations, and difficulty with daily tasks. Complication: Parkinson’s disease dementia. Management: Rivastigmine (first-line cholinesterase inhibitor); review dopaminergic drugs that worsen hallucinations.
- Case 4 - Autonomic Dysfunction 💧: A 70-year-old woman with PD reports frequent faints on standing, constipation, and urinary urgency. BP falls from 135/80 supine to 95/60 standing. Complication: Autonomic dysfunction (orthostatic hypotension, bladder involvement). Management: Non-pharmacological (slow position changes, compression stockings, ↑ salt/fluid); consider fludrocortisone or midodrine.
- Case 5 - Impulse Control Disorder 🎰: A 60-year-old man on pramipexole for PD develops compulsive gambling and hypersexuality, which his wife finds distressing. Complication: Dopamine agonist–induced impulse control disorder. Management: Reduce/stop dopamine agonist; switch to levodopa-based regimen; behavioural support.
Teaching Commentary 🧠
Parkinson’s disease complications can be divided into: - Motor: fluctuations (“wearing off”), dyskinesias. - Neuropsychiatric: dementia, hallucinations, depression, impulse control disorders. - Autonomic: postural hypotension, constipation, bladder dysfunction, erectile dysfunction. - Sleep: REM sleep behaviour disorder, insomnia. Complications often reflect both disease progression and treatment side effects. Management requires balancing dopaminergic therapy, adding adjuncts (COMT/MAO-B inhibitors), and addressing non-motor symptoms with MDT support. Deep brain stimulation is an option in selected patients with refractory motor fluctuations.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery