
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
ECG Reading & Interpretation MLA and Exams 🫀
Related Subjects: |ECG Basics |ECG Axis |ECG Analysis |ECG LAD |ECG RAD |ECG Low voltage |ECG Pathological Q waves |ECG ST/T wave changes |ECG LBBB |ECG RBBB |ECG short PR |ECG Heart Block |ECG Asystole and P wave asystole |ECG QRS complex |ECG ST segment |ECG: QT interval |ECG: LVH |ECG RVH |ECG: Bundle branch blocks |ECG Dominant R wave in V1 |ECG Acute Coronary Syndrome |ECG Crib sheets
💡 ECGs for the MLA Medical students should be able to recognise key ECG patterns in acute and chronic disease, linking them to underlying pathology and urgent management steps.
1. Basics of ECG
An ECG (electrocardiogram) records the heart's electrical activity. It uses 10 electrodes to produce 12 leads, each giving a different perspective of the heart.
📌 Key Points:
- Leads I, II, III → Limb leads (frontal plane)
- aVR, aVL, aVF → Augmented limb leads
- V1–V6 → Chest leads (horizontal plane)
- Each lead “views” the heart from a different angle
2. Systematic ECG Approach
Step 1: Rate 🏃♂️
Normal sinus rhythm: 60–100 bpm. Quick method: 300 ÷ number of large squares between R waves.
Step 2: Rhythm 🧭
- Check if rhythm is regular or irregular
- Look for P waves: Are they present and consistent?
- PR interval: Normal 120–200 ms (3–5 small squares)
Step 3: Axis 📐
Determine QRS axis in frontal leads:
- Normal: -30° to +90°
- Left axis deviation: -30° to -90°
- Right axis deviation: +90° to +180°
Step 4: Intervals ⏱️
- PR interval: 120–200 ms
- QRS duration: < 120 ms
- QT interval: Rate-corrected using Bazett's formula (QTc)
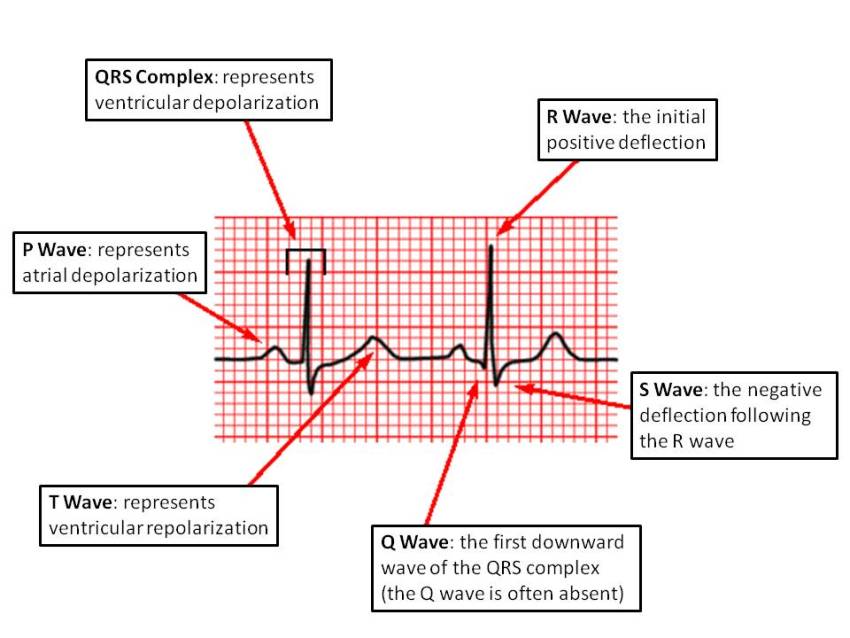
Step 5: Waveform Morphology 🔍
- P wave → Atrial depolarization
- QRS complex → Ventricular depolarization
- T wave → Ventricular repolarization
- ST segment → Look for elevation/depression (ischemia or infarction)
- U wave → Often seen in hypokalemia
3. Common ECG Patterns
| Condition | ECG Features | Teaching Tip |
|---|---|---|
| Sinus Bradycardia | Rate < 60 bpm, normal P-QRS-T | Usually benign unless symptomatic |
| Sinus Tachycardia | Rate > 100 bpm, normal morphology | Look for underlying cause: fever, hypovolemia, pain |
| AF (Atrial Fibrillation) | Irregularly irregular, no distinct P waves, fibrillatory baseline | Check for thromboembolic risk (CHA₂DS₂-VASc) |
| STEMI | ST elevation in contiguous leads, reciprocal changes | Correlate with clinical chest pain → urgent reperfusion |
| Bundle Branch Block | QRS ≥120 ms, specific V1/V6 patterns for RBBB/LBBB | Can mask MI; recognise morphology carefully |
4. Practical Tips 🧠
- Always correlate ECG with clinical context
- Check patient identity, calibration, and lead placement
- Compare with previous ECGs for changes
- Look for electrolyte disturbances and drug effects
🫀 Introduction to ECGs
Why ECGs matter: ECGs translate cardiac electricity into patterns you can learn. Start every trace the same way: calibration → rate → rhythm → axis → intervals → waveforms/segments → compare with old.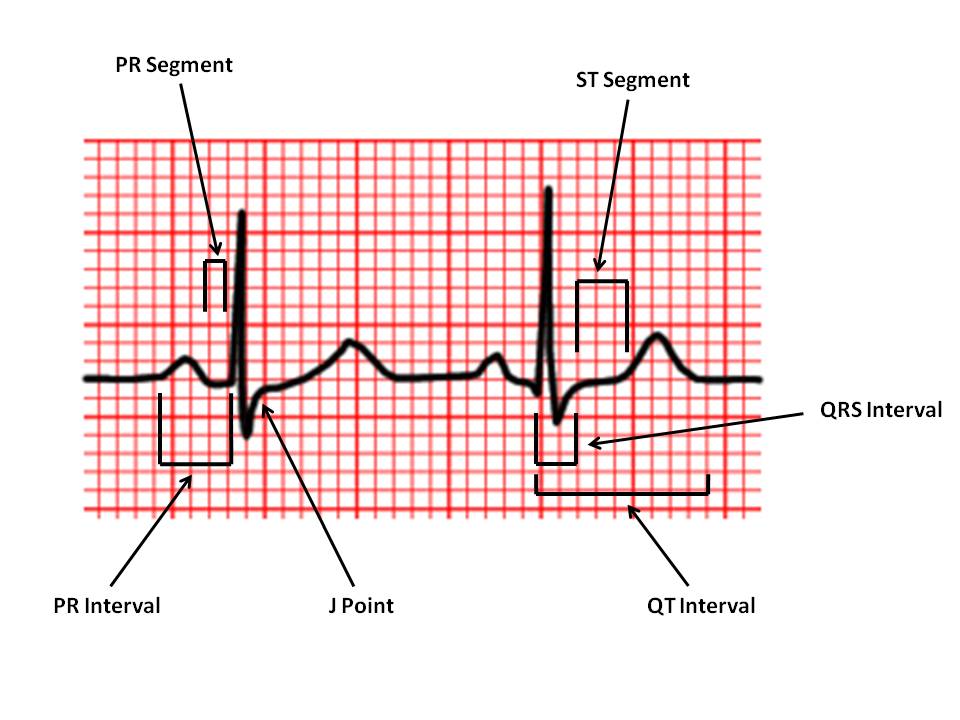
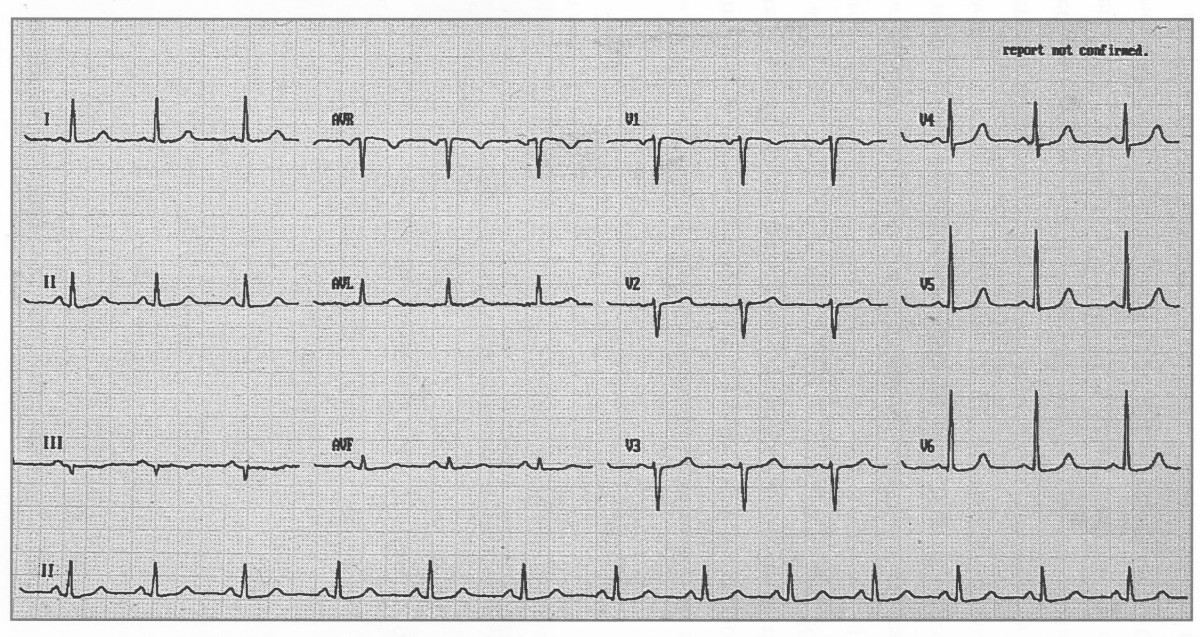
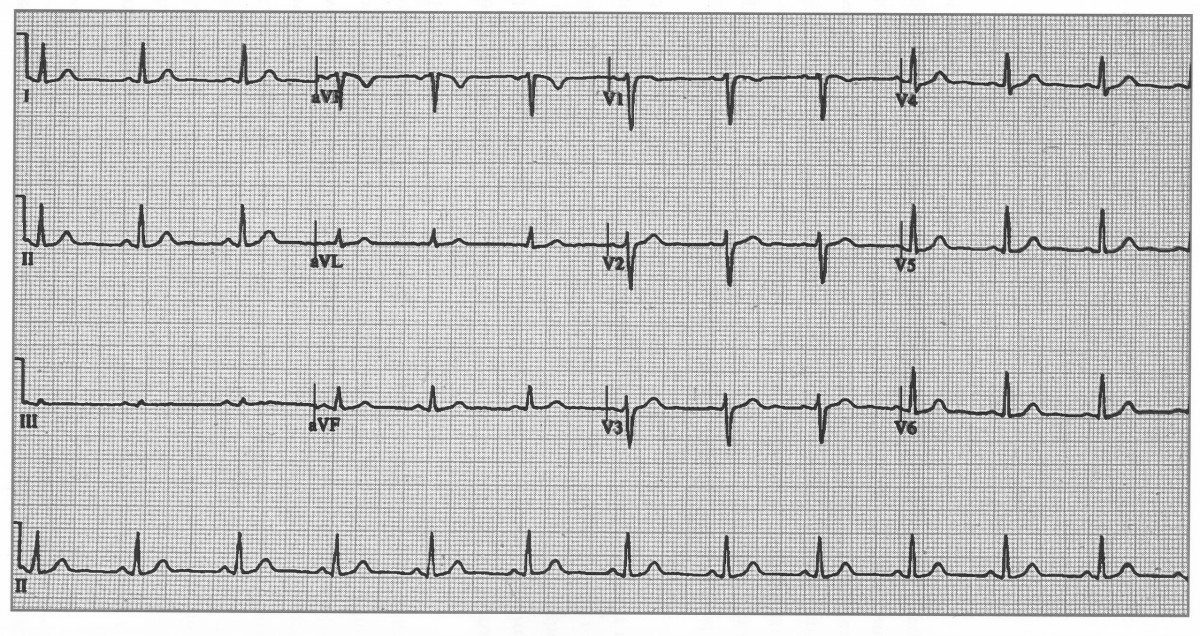
✅ Normal ECGs
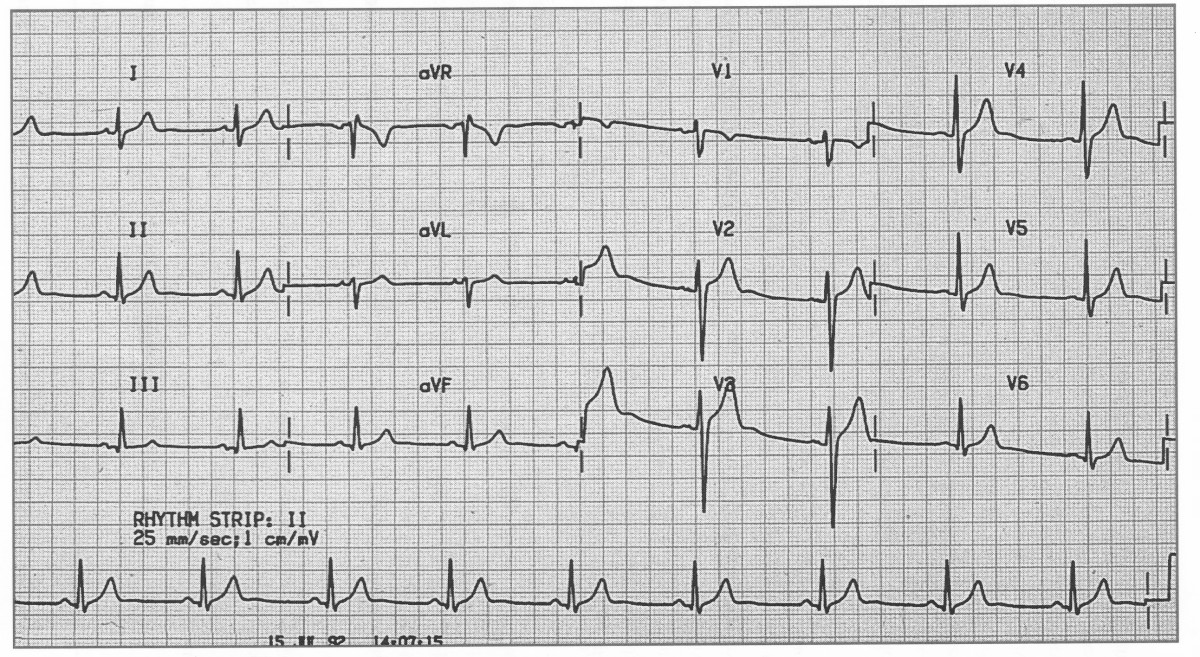
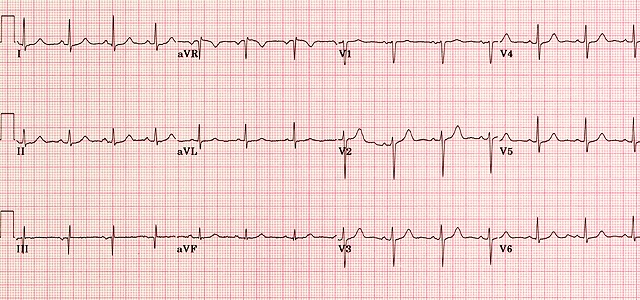
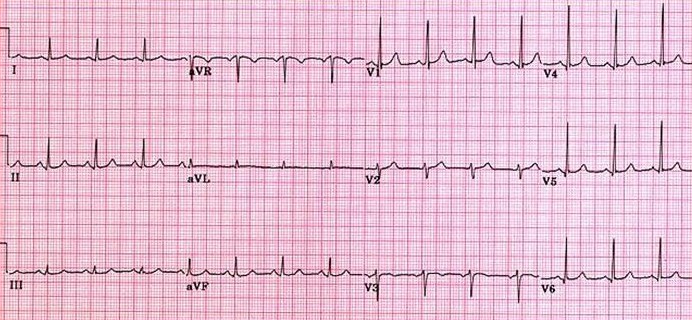
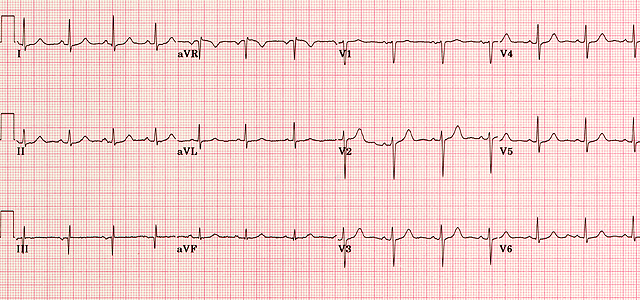
Annotated normal ECG. Sinus rhythm 60–100 bpm (this one ≈82), normal PR/QRS/QT, isoelectric ST.
🧭 The 7-Step ECG Reading Method (teach & test)
- Calibration & quality 📏 - Confirm 25 mm/s and 10 mm/mV; check artefact and lead placement (V1–V6 positions).
- Rate ⏱️ - Regular rhythm: 300-150-100-75-60-50 (big-box method). Irregular: count complexes in 10 s strip ×6.
- Rhythm 🔄 - P before every QRS? Constant PR? Narrow vs wide QRS? Sinus = upright P in I/II/aVF, negative in aVR.
- Axis 🧭 - Normal ≈ −30° to +90°. Quick check: Lead I & aVF both positive → normal; I positive / aVF negative → left axis; I negative / aVF positive → right axis.
- Intervals 📐 - PR 120–200 ms; QRS ≤120 ms; QTc <440 ms (men), <460 ms (women). Use Bazett (QT/√RR) or Fridericia (QT/∛RR) if brady/tachy.
- Waves/segments 🌊 - P (morphology, P pulmonale/mitrale), QRS (hypertrophy, bundle blocks), ST (↑/↓), T (inversions, hyperacute), U waves (hypokalaemia).
- Compare 🗂️ - With prior ECGs and clinic context (pain, K+, troponin, meds like digoxin). UK practice: document “ECG unchanged vs prior”.
📏 Normal Ranges (quick reference)
| Feature | Normal | Notes |
|---|---|---|
| P wave | ≤110 ms, ≤2.5 mm height | Upright I/II/aVF, negative aVR; V1 often biphasic. |
| PR interval | 120–200 ms | Short PR: pre-excitation; long PR: AV block 1°. |
| QRS duration | ≤120 ms | Look for RBBB/LBBB patterns, delta waves. |
| QRS voltage | ≥5 mm limb lead OR ≥10 mm precordial | High voltage ≠ always LVH; check criteria + repolarisation. |
| QTc | <440 ms (M), <460 ms (F) | Correct for rate; avoid Bazett in extremes (consider Fridericia). |
| Axis | −30° to +90° | Age and body habitus influence axis. |
🧪 Pattern recognition (must-know)
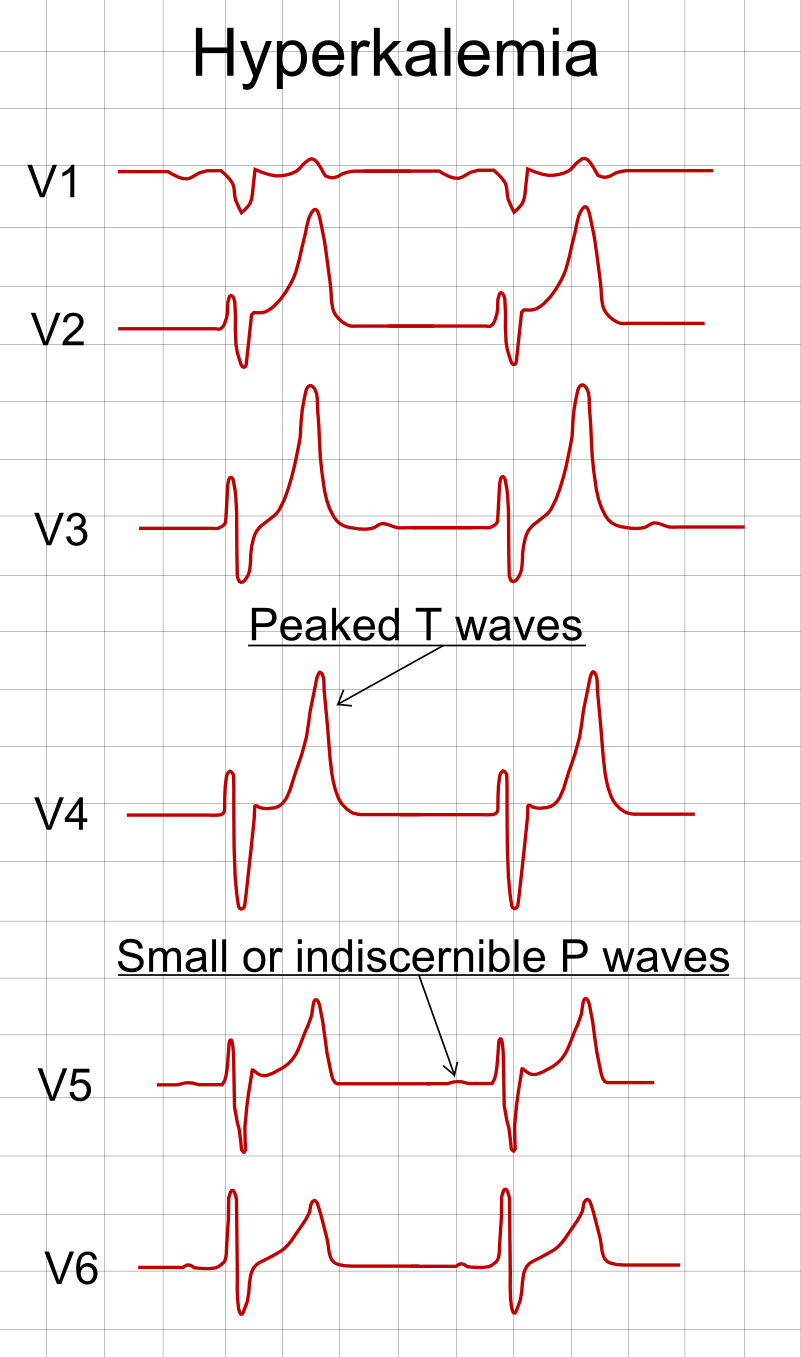
- Hyperkalaemia 🔺K⁺ - Tall, peaked T; PR prolongation; QRS widening → sine-wave. Urgent calcium gluconate.
- Hypokalaemia 🔻K⁺ - Flat T, U waves, prolonged QT → torsades risk.
- Pericarditis ♨️ - Diffuse concave ST↑ with PR↓; reciprocal PR↑ in aVR; no localised reciprocal ST↓.
- STEMI ❤️🔥 - J-point ST↑ in contiguous leads (limb ≥1 mm; V2–V3 sex/age cut-offs). Look for reciprocal ST↓. New LBBB with ischaemic symptoms → treat as STEMI.
- Wellens’ ⚠️ - Deep/biphasic T in V2–V3 pain-free → critical LAD; avoid stress testing; cardiology review.
- Brugada 🧬 - Coved ST↑ V1–V3 with RBBB-like pattern → refer; fever can unmask.
- PE 🫁 - Sinus tachy, S1Q3T3, RBBB/Right axis; not sensitive-use clinical pre-test + D-dimer/CTPA.
🧠 AV & Bundle Branch Blocks (pattern drill)
| Block | ECG | Pearl |
|---|---|---|
| 1° AV | PR >200 ms, every P conducts | Often benign; watch with β-blockers, CCB, digoxin. |
| Mobitz I (Wenckebach) | PR progressively ↑ then drop | Usually AV-nodal; often transient (e.g., inferior MI). |
| Mobitz II | Fixed PR with dropped QRS | Infranodal; risk of complete heart block → pacing. |
| 3° AV (complete) | AV dissociation; escape rhythm | Unstable → atropine/chronotrope; likely pacemaker. |
| RBBB | V1 rsR′, wide S in I/V6 | May be normal variant; consider PE/ischaemia. |
| LBBB | Broad/notched R in I/V5–6, absent Q in lateral leads | Mask ischaemia; use clinical picture (Sgarbossa/Smith-mod). |
🛠️ Quick how-to: calculate rate
- Regular: 300/150/100/75/60/50 big-box method (R-R distance).
- Irregular: Count QRS in 10-second strip ×6 (or 6-second hash marks ×10).
🩺 UK exam & practice tips
- Document calibration, rate, rhythm, axis, intervals, abnormalities, and comparison: “ECG: 25 mm/s, 10 mm/mV; SR 78; normal axis; PR 160 ms; QRS 90 ms; QTc 420 ms; no ST-T changes; unchanged from 2023.”
- STEMI criteria follow UK pathways (J-point thresholds + symptoms). Don’t miss posterior MI (V7–V9) if V1–V3 ST↓ with tall R. 🚩
- Always interpret ECG in clinical context-ECG cannot “rule out” MI without symptoms/troponin. 🔬
A normal ECG shows: - Regular sinus rhythm - Appropriate rate, axis, intervals, voltages, and morphology - No pathological Q waves, ST/T changes, conduction defects, hypertrophy, or arrhythmia Normal ranges are for resting adults (≥16 y); variations exist in children, athletes, pregnancy, ethnicity, body habitus.
Systematic Interpretation Checklist
- Rate: 60–100 bpm
- Rhythm: Sinus (P before every QRS, consistent PR, upright P in II)
- Axis: –30° to +90° (normal); physiological left axis –30° to –90° common
- Intervals: PR 120–200 ms, QRS ≤110 ms (≤120 ms acceptable), QTc ≤440 ms (men), ≤460 ms (women)
- P waves: Upright I/II/aVF, ≤2.5 mm amplitude, ≤120 ms duration
- QRS voltage & morphology: Normal progression (small R V1 → large R V5/V6), no pathological Q waves
- ST segment: Isoelectric or minimal elevation/depression (<1 mm)
- T waves: Concordant with QRS, upright I/II/V3–V6, inverted aVR
- U waves: Absent or small (<1 mm) in V2–V3
Detailed Normal Values & Features
| Parameter | Normal Range (Adults) | Notes / Variations |
|---|---|---|
| Rate | 60–100 bpm | Sinus bradycardia <60 (common in athletes); tachycardia >100 |
| Rhythm | Sinus rhythm | P wave before QRS, PR constant, P positive in II |
| P wave | Duration ≤120 ms
Amplitude ≤2.5 mm (limb leads) |
Upright I, II, aVF; biphasic V1 (positive then negative); no notching |
| PR interval | 120–200 ms | Shorter in young/athletes; longer in elderly (up to 220 ms still normal) |
| QRS duration | ≤110 ms (≤120 ms acceptable) | Narrow complex; no BBB, WPW (delta wave), or fascicular block |
| QRS axis | –30° to +90° | Left axis deviation –30° to –90° physiological (obesity, pregnancy, ascites) |
| QRS voltage | Limb: R ≤20 mm, S ≤15 mm
Precordial: R V5/V6 ≤27 mm, S V1/V2 ≤30 mm |
No low voltage (<5 mm limb leads) or high voltage (LVH criteria) |
| R-wave progression | Small R V1 → transition V3–V4 → tall R V5/V6 | Poor progression can be normal in obesity/COPD |
| ST segment | Isoelectric (±0.5 mm) | Early repolarisation: concave upward elevation (1–3 mm) in V2–V5 common in young males |
| T wave | Upright I, II, V3–V6; inverted aVR | Concordant with QRS; amplitude <5 mm limb, <10 mm precordial; no deep inversion |
| QTc (Bazett) | ≤440 ms men, ≤460 ms women | Upper limit ~450–470 ms; shorter in hypercalcaemia, longer in drugs/hypokalaemia |
| U wave | Absent or small (<1 mm) after T in V2–V3 | Prominent U waves abnormal (hypokalaemia, drugs) |
Normal Variants (Not Abnormal)
- Early repolarisation: Concave ST elevation (1–4 mm) in V2–V5, notched/slurred J point, tall T waves – common in young, black males, athletes
- Sinus arrhythmia: Rate variation with respiration (increases on inspiration) – normal in young/athletes
- Persistent juvenile T-wave pattern: T inversion V1–V3 (sometimes V4) – normal in young adults, especially women
- Wandering atrial pacemaker: Slight P-wave morphology change with rate variation – benign
- Borderline axis: –30° to –45° or +90° to +110° – often normal
Common Pitfalls & When to Call Abnormal
- Pathological Q waves: ≥0.04 s wide or ≥25% R-wave depth in ≥2 contiguous leads
- ST elevation: ≥1 mm limb leads or ≥2 mm precordial (men <40 y), ≥1.5 mm women – consider STEMI/early repolarisation
- ST depression: ≥0.5 mm horizontal/downsloping – ischaemia
- Left axis deviation < –30° or right > +90° – consider conduction defect
- Prolonged QTc >470–500 ms – risk of TdP
- Low voltage + electrical alternans – pericardial effusion
Clinical Pearls (Exam/OSCE/MCQ)
- Report systematically: "Rate, rhythm, axis, intervals, ST/T changes, voltage, progression"
- Always compare to previous ECGs if available
- Normal ECG does NOT exclude acute ischaemia (up to 20–30% NSTEMI have normal ECG)
- Athletes often have sinus bradycardia, early repolarisation, high voltages – physiological
- Ethnic variations: Higher voltage and early repolarisation more common in black individuals
- Age: PR/QRS slightly longer in elderly; T inversion V1–V2 more common in women
Sources (2025–2026)
- AHA/ACC/HRS: ECG Standardization & Interpretation (2009, reaffirmed 2025)
- ESC Guidelines: Acute Coronary Syndromes (2023–2025)
- Life in the Fast Lane ECG Library (updated 2025)
- Marriott's Practical Electrocardiography (13th ed.)
- UpToDate: ECG Interpretation (2026)