Related Subjects:
|Nikolsky's sign
|Koebner phenomenon
|Psoriatic Arthritis
|Psoriasis
|Eczema/Dermatitis
|Anatomy of Skin
| Topical Steroids
🧴 Topical corticosteroids (topical steroids) - a practical UK guide
Topical corticosteroids are anti-inflammatory medicines applied to the skin to rapidly reduce erythema, itch, oedema, and scaling in steroid-responsive dermatoses (especially eczema and psoriasis). They bind intracellular glucocorticoid receptors and downregulate pro-inflammatory gene transcription (cytokines, adhesion molecules), while also causing superficial vasoconstriction - so redness and itch often improve quickly. The clinical skill is matching potency to (1) severity and diagnosis, (2) body site/skin thickness, and (3) age, then stepping down once controlled to minimise harm while maintaining barrier repair with emollients.
✅ When to use
- 🧒 Eczema flares (atopic, discoid, contact): reduce inflammation + itch → restore barrier and break the itch–scratch cycle.
- 🧩 Psoriasis (selected sites): reduce plaque inflammation and scaling (often paired with vitamin D analogues or keratolytics in practice).
- 🐜 Inflammatory bite reactions / lichen simplex (short courses): symptomatic control.
- 🚫 Not a moisturiser: steroids treat inflammation; emollients treat dryness/barrier dysfunction.
🎯 Choosing potency: site + age + severity
- 👁️ Face/eyelids/genitals/flexures: usually mild → moderate, short courses (higher absorption, higher atrophy risk).
- 🦶 Palms/soles or lichenified plaques: often need potent for short periods.
- 👶 Children: higher surface-area-to-weight ratio → greater systemic absorption risk; use the lowest effective potency and review early.
- 🩹 Occlusion (dressings, cling film): can massively increase absorption - use only if specifically advised.
🧠 How to apply (the “right place, right amount, right time” rule)
- 📍 Apply to inflamed skin only (red/itchy/thickened), in a thin shiny layer.
- 🗓️ Once daily is often enough for many preparations; follow product/local guidance and reassess response.
- 🧴 Keep emollients generous and regular; separate applications (commonly 20–30 minutes) to avoid dilution/spread.
- 🧼 Wash hands after (unless treating hands), avoid eyes/mucosa.
📏 Fingertip unit (FTU) - simple dosing that prevents under-treatment
Under-application is a common reason steroids “don’t work”. Teach FTUs early: it improves adherence, safety, and outcomes.
| FTU concept |
What it means in practice |
| 👆 1 FTU |
A line of cream/ointment from fingertip to first finger crease (adult index finger). Roughly 0.5 g. |
| 🖐️ Coverage guide |
About 2 adult handprints of skin (front + back of one hand area). |
| ✅ Why it matters |
Helps patients use enough to control inflammation, without escalating potency unnecessarily. |
🪜 Duration and step-down strategy (how to stay safe)
- 🔥 Treat flares decisively, then step down (reduce potency and/or frequency) once controlled.
- 🧩 If it rebounds quickly, think: diagnosis wrong? adherence/FTU? infection? contact allergy? need steroid-sparing therapy?
- 🧴 Maintenance is mostly emollients + trigger control; some patients use intermittent “proactive” regimens (protocol/specialist-led).
⚠️ Adverse effects (and how good prescribing prevents them)
- 🧻 Local: skin atrophy (thin, shiny skin), striae, telangiectasia, purpura/bruising, acne/rosacea flares, perioral dermatitis, delayed healing.
- 🦠 Infection: can mask/worsen fungal, bacterial, viral infection (e.g. tinea incognito) - reassess if painful, crusted, rapidly spreading, or not improving.
- 👁️ Peri-ocular risk: prolonged eyelid use can contribute to glaucoma/cataract risk - keep short and cautious.
- 🧠 Systemic (rare but important): HPA-axis suppression / Cushingoid effects - risk rises with high potency, large areas, prolonged use, occlusion, and in children.
🚩 Red flags for review / referral
- ⏳ No improvement after an appropriate course with correct FTU dosing.
- 😣 Painful erosions, extensive weeping/crusting, systemic unwellness, or suspected eczema herpeticum (urgent same-day assessment).
- 🔁 Repeated need for very potent steroids, large-area use, or long-term face/genital steroid use.
- ❓ Diagnostic uncertainty (eczema vs psoriasis vs tinea): wrong diagnosis drives escalation and harm.
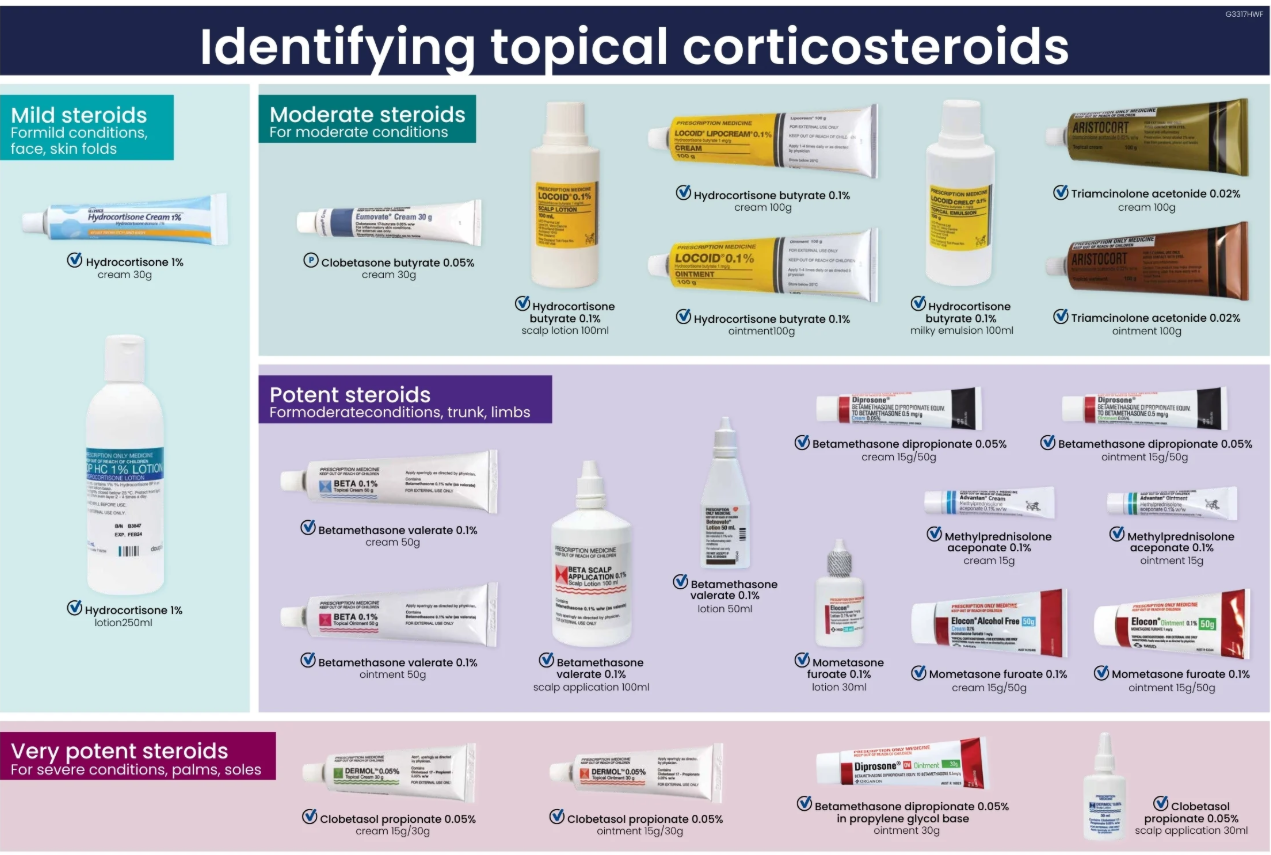
📚 Types of topical steroids by potency (UK examples)
Potency groupings are commonly listed as mild, moderate, potent, and very potent in UK formularies. The examples below reflect typical UK preparations; exact classification can vary by reference and formulation.
| Potency |
Generic |
Strength |
Common UK brand examples |
Typical use notes |
| 💥 Very potent |
Clobetasol propionate |
0.05% |
Dermovate |
Short courses; avoid face/flexures unless specialist advice. |
| 💪 Potent |
Betamethasone valerate |
0.1% |
Betnovate |
Trunk/limbs; lichenified eczema/psoriasis flares. |
| 💪 Potent |
Mometasone furoate |
0.1% |
Elocon |
Often once daily; avoid prolonged face use. |
| 💪 Potent |
Fluticasone propionate |
0.005% cream / 0.05% ointment |
Cutivate |
Potency depends on formulation; choose by site/severity. |
| 💪 Potent |
Fluocinolone acetonide |
0.025% |
Synalar |
Useful for inflammatory dermatoses; review if recurrent use. |
| 💪 Potent |
Beclometasone dipropionate |
0.025% |
(varies by product) |
Potency classification can vary; follow local formulary. |
| 🙂 Moderate |
Clobetasone butyrate |
0.05% |
Eumovate / Clobavate |
Good “middle option” for mild–moderate eczema flares. |
| 🙂 Moderate |
Betamethasone valerate |
0.025% |
Betnovate-RD |
Often used as a step-down from potent therapy. |
| 🌿 Mild |
Hydrocortisone |
0.5%–2.5% |
e.g. Hydrocortisone 1% cream; Dermacort / Dioderm (brand varies) |
Face/flexures; short courses; good first-line for mild inflammation. |
| 🌿 Mild |
Fluocinolone acetonide |
0.0025% |
Synalar 1 in 10 |
Mild option; review response and avoid long unreviewed use. |
🗣️ Patient counselling (a one-minute script)
- 🧴 “Use your emollient every day - it prevents flares.”
- 🎯 “Use the steroid only on red/itchy patches, in the right FTU amount.”
- 🪜 “Once it’s clear, we step down or stop - don’t keep using it daily for weeks without review.”
- 🚩 “Come back if it’s painful, crusting, spreading, or not improving - it may be infection or a different diagnosis.”
📌 Reference
- BNF. Topical corticosteroids (Topical steroids). Adapted list of examples and strengths (Accessed January 2022).