Related Subjects:
|Iron deficiency Anaemia
|Haemolytic anaemia
|Macrocytic anaemia
|Megaloblastic anaemia
|Microcytic anaemia
|Myelodysplasia
|Myelofibrosis
|Hereditary Spherocytosis
|Hereditary Elliptocytosis
|Haemophilia A
|Haemophilia B
|Haemolytic anaemia
|Heme
|Globins
|Red blood cells
|White blood cells
|Lymphocytes
|Platelets
|Cryoprecipitate
|Fresh Frozen Plasma
|Blood Cell Maturation
|Blood film interpretation
|Reticulocytes
🧬 Malignant haematological condition characterised by ineffective haematopoiesis, cytopenias, and a risk of transformation into acute myeloid leukaemia (AML).
Key Point: Median survival is < 2 years in many subtypes, with infection and bleeding being the most common causes of death. ⚠️
📖 About
- Myelodysplastic syndrome (MDS) is a pre-leukaemic clonal disorder of dysplastic haemopoietic stem cells.
- Occurs mainly in older adults (rare under age 55).
- Progressive, with median survival depending on subtype and cytogenetic abnormalities.
- Transformation to AML occurs in 20–30% of patients.
🧬 Aetiology
- ~80% of patients have identifiable genetic/cytogenetic abnormalities.
- Maturation block → pancytopenia and ineffective haematopoiesis.
- Affects all myeloid lineages, with accumulation of blasts in the marrow.
- Marrow blast % = most important prognostic factor (≥20% = AML).
👶 Commoner in association with:
- Inherited bone marrow failure syndromes:
- Down syndrome
- Fanconi anaemia
- Bloom syndrome
- Ataxia telangiectasia
- Shwachman-Diamond syndrome
- Secondary causes:
- Previous chemotherapy or radiotherapy (therapy-related MDS)
- Chemical exposure (e.g., benzene, pesticides)
📊 WHO Classification of MDS
| Disease | Bone marrow findings |
|---|
| MDS with single-lineage dysplasia | < 5% blasts; dysplasia confined to one lineage |
| MDS with ring sideroblasts (MDS-RS) | >15% ring sideroblasts, or 6–14% with SF3B1 mutation |
| MDS with multilineage dysplasia | < 5% blasts; dysplasia in ≥2 lineages |
| MDS with excess blasts | 5–19% blasts |
| MDS with isolated del(5q) | < 5% blasts; del(5q) cytogenetic abnormality; often ↑ platelets |
| MDS, unclassifiable | Does not fit above categories or inadequate marrow material |
🩺 Clinical Features: Progressive Bone Marrow Failure
- Anaemia: Fatigue, pallor, dyspnoea.
- Leucopenia: Recurrent infections (neutropenia + neutrophil dysfunction).
- Thrombocytopenia: Petechiae, purpura, mucosal bleeding.
- Bone marrow expansion: Rarely bone pain.
- Death is usually due to infection or haemorrhage.
🔍 Investigations
- FBC: Pancytopenia (low Hb, WCC, platelets).
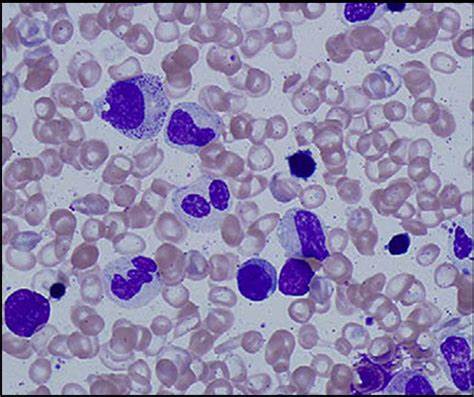
- Blood film: Dysplastic features – macrocytosis, hypogranular neutrophils, pseudo–Pelger-Huët anomaly.
- Bone marrow biopsy: Hypercellular marrow with dysplasia. >20% blasts = AML.
- Genetics: Abnormalities of chromosomes 5q, 7q, or complex karyotypes.
- Biochemistry: No reticulocytosis (ineffective erythropoiesis).
💊 Management (Prognosis often poor)
- Supportive care: RBC and platelet transfusions, antibiotics.
- Erythropoietin: May improve anaemia in some patients.
- G-CSF: Can boost neutrophil counts, especially with EPO.
- Lenalidomide: Effective in MDS with isolated del(5q).
- Azacitidine: Hypomethylating agent, prolongs survival in high-risk MDS (~9 months benefit).
- Allogeneic stem cell transplant: Only curative option, suitable for young fit patients.
- Chemotherapy: Occasionally used in high-risk or transforming disease.
📚 References
Cases - Myelodysplastic Syndrome (MDS)
- Case 1 - Incidental Cytopenia in Elderly:
A 76-year-old man is found to have anaemia on a routine check (Hb 9.5 g/dL, MCV 105 fL). WCC and platelets are normal. Blood film shows macrocytosis with dysplastic neutrophils. Bone marrow: hypercellular with dysplastic erythroid precursors. Diagnosis: MDS with isolated anaemia.
- Case 2 - Pancytopenia with Infections:
A 70-year-old woman presents with recurrent chest infections and bruising. FBC: Hb 8.9 g/dL, WCC 2.5 ×10⁹/L, platelets 70 ×10⁹/L. Film shows hypogranular neutrophils and anisopoikilocytosis. Bone marrow: trilineage dysplasia. Diagnosis: MDS presenting with pancytopenia.
- Case 3 - Macrocytic Anaemia Misdiagnosed as B12 Deficiency:
A 68-year-old man with fatigue is treated for “B12 deficiency” but fails to improve despite supplementation. Hb 9.0 g/dL, MCV 108 fL, normal B12/folate. Film: dysplastic neutrophils with pseudo–Pelger-Huët anomaly. Diagnosis: MDS mimicking megaloblastic anaemia.
- Case 4 - Transformation Risk:
A 65-year-old woman with known low-risk MDS is followed in clinic. Over 18 months, her blast count increases from 3% to 18%. She develops worsening anaemia and thrombocytopenia. Diagnosis: High-risk MDS with progression towards acute myeloid leukaemia (AML).
- Case 5 - Secondary (Therapy-Related) MDS:
A 60-year-old man treated with chemotherapy and radiotherapy for Hodgkin lymphoma 7 years ago presents with fatigue and bruising. FBC: Hb 8.7 g/dL, WCC 3.0 ×10⁹/L, platelets 55 ×10⁹/L. Bone marrow: dysplasia with cytogenetic abnormalities (del(5q), monosomy 7). Diagnosis: Therapy-related MDS.
Teaching Commentary 🧬
Myelodysplastic syndromes are clonal bone marrow disorders causing ineffective haematopoiesis and risk of transformation to AML. They typically affect older adults. Clinical features: anaemia, infections, bruising/bleeding. Labs: macrocytosis, cytopenias, dysplastic neutrophils (e.g. pseudo–Pelger-Huët cells), and abnormal marrow morphology.
Risk stratification is via IPSS-R score (cytogenetics, blasts, cytopenias). Management ranges from supportive (transfusions, erythropoietin) to disease-modifying (azacitidine, lenalidomide in 5q-), and allogeneic stem cell transplant in selected younger patients. Always suspect therapy-related MDS in patients with prior chemo/radiotherapy.
