
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Community Acquired Pneumonia 🫁 ✅
Related Subjects: Asthma |Acute Severe Asthma |Exacerbation of COPD |Pulmonary Embolism |Cardiogenic Pulmonary Oedema |Pneumothorax |Tension Pneumothorax |Respiratory (Chest) infections Pneumonia |Fat embolism |Hyperventilation Syndrome |ARDS |Respiratory Failure |Diabetic Ketoacidosis |Lung Empyema
Community-acquired pneumonia (CAP) is an acute infection of the lung parenchyma acquired outside hospital and appears within 48 hours of admission. It causes inflammation of the alveoli and interstitium, producing consolidation, impaired gas exchange, and systemic illness. In UK practice, the priorities are to recognise CAP early, assess severity, start appropriate antibiotics promptly, and identify complications or alternative diagnoses.
📖 About CAP
- CAP usually presents with acute cough, fever, breathlessness, and new focal chest signs.
- It ranges from mild illness managed in the community to severe sepsis and respiratory failure requiring critical care.
- Older age, frailty, chronic lung disease, smoking, alcohol excess, and immunocompromise increase risk of severe disease.
🧬 Microbiology of CAP
- Streptococcus pneumoniae — most common typical cause
- Haemophilus influenzae — more common in COPD, smokers and older adults
- Respiratory viruses — influenza, RSV, SARS-CoV-2 and others
- Mycoplasma pneumoniae — atypical pneumonia, often younger patients/outbreaks
- Staphylococcus aureus — consider after influenza or in severe pneumonia
- Chlamydia psittaci — psittacosis; bird exposure
- Coxiella burnetii — Q fever; farm animals/parturient livestock exposure
- Legionella pneumophila — severe CAP, travel/hotel exposure, hyponatraemia
🧬 Pathophysiology
- Micro-organisms reach the distal airways, usually by microaspiration of colonising upper-airway organisms.
- Local host defences are overcome, leading to alveolar inflammation and accumulation of inflammatory exudate.
- This causes consolidation, reduced ventilation of affected lung units, and V/Q mismatch with hypoxaemia.
- Systemic inflammation may cause fever, tachycardia, delirium, hypotension, and sepsis.
🔎 Types of Pneumonia (Pathology)
- 🌑 Lobar Pneumonia: Entire lobe affected, usually S. pneumoniae. Pathological progression through 4 stages (see below).
- 🟡 Bronchopneumonia: Patchy, often basal consolidation spreading from bronchioles. Elderly, bedridden, aspiration-prone.
- 🌫️ Interstitial (Atypical): Alveolar septal inflammation; usually viral (influenza, RSV) or atypical bacteria (Mycoplasma).
- 🟢 Necrotising Pneumonia: Severe destruction ± abscess (e.g. S. aureus, Klebsiella).
- 🦠 Opportunistic: Pneumocystis jirovecii in AIDS, fungal pneumonias (Aspergillus, Cryptococcus).
📆 Classical Stages of Lobar Pneumonia
- 1️⃣ Congestion (Day 1–2): Heavy, red lung. Vascular engorgement, intra-alveolar fluid, few neutrophils, numerous bacteria.
- 2️⃣ Red Hepatization (Day 3–4): Firm, liver-like lung. Alveoli packed with neutrophils, RBCs, fibrin → red, airless tissue.
- 3️⃣ Gray Hepatization (Day 5–7): RBC breakdown → gray-brown tissue. Dense fibrinopurulent exudate, neutrophil dominance.
- 4️⃣ Resolution (Day 8+): Enzymatic digestion, macrophage clearance → lung architecture restored (or scarred if incomplete).
🧫 Histopathology
- Lobar Pneumonia: Intra-alveolar neutrophilic infiltrate, fibrin, RBCs. Thickened alveolar septa. Exudate fills airspaces.
- Bronchopneumonia: Suppurative inflammation centred on bronchi/bronchioles, patchy consolidation.
- Interstitial Pneumonia: Mononuclear infiltrates (lymphocytes, macrophages) in alveolar walls; airspaces often clear.
- Viral Pneumonia: Cytopathic effects (giant cells in RSV, inclusion bodies in CMV).
- Pneumocystis jirovecii: Foamy intra-alveolar exudate, cup-shaped organisms on silver stain.
⚠️ Risk factors
- Older age and frailty
- Chronic respiratory disease (for example COPD or bronchiectasis)
- Smoking and excess alcohol
- Neurological disease, aspiration risk, poor swallow
- Immunosuppression
- Diabetes, heart failure, chronic kidney disease, chronic liver disease
🩺 Clinical features
- Fever, rigors, sweats, Cough, with or without sputum
- Breathlessness, Pleuritic chest pain
- New focal chest signs such as crackles, bronchial breathing, or reduced air entry
- Systemic upset, reduced exercise tolerance, anorexia
- Older adults may present atypically with confusion, falls, or functional decline
🔍 Differential Diagnosis of CAP
- Pulmonary embolism — pleuritic chest pain, haemoptysis, tachycardia, hypoxia or risk factors for VTE
- Acute heart failure / cardiogenic pulmonary oedema — bilateral crackles, raised JVP, peripheral oedema, orthopnoea or high BNP/NT-proBNP
- Acute bronchitis — cough without focal chest signs or new consolidation on chest X-ray
- Asthma or COPD exacerbation — wheeze, known obstructive lung disease, increased sputum or reduced peak flow
- Pneumothorax — sudden pleuritic pain, unilateral reduced breath sounds and hyper-resonance
- Lung malignancy — especially with haemoptysis, weight loss, smoking history or non-resolving focal consolidation
- Interstitial lung disease / organising pneumonia — subacute breathlessness, dry cough, diffuse crackles or persistent inflammatory infiltrates
- Aspiration pneumonitis / aspiration pneumonia — dysphagia, reduced consciousness, vomiting, neurological disease or frailty
- Tuberculosis — chronic cough, night sweats, weight loss, haemoptysis or relevant exposure/travel history
📊 Severity assessment
- Use clinical judgement together with a validated severity score.
- In adults, CURB-65 is commonly used:
- Confusion
- Urea >7 mmol/L
- Respiratory rate ≥30/min
- Blood pressure: systolic <90 mmHg or diastolic ≤60 mmHg
- Age 65 or over
- Higher scores suggest greater mortality risk and are used to help decide on hospital admission and treatment intensity.
- Do not rely on CURB-65 alone; oxygen requirement, frailty, comorbidity, sepsis, and social factors also matter.
🚑 When to admit
- Moderate or high severity CAP
- Hypoxaemia or respiratory distress
- Sepsis or haemodynamic instability
- Inability to take oral therapy or maintain hydration
- Significant frailty, delirium, or poor support at home
- Diagnostic uncertainty or concern about complications
🔎 Investigations
- Observations: respiratory rate, oxygen saturation, pulse, blood pressure, temperature, mental state
- Chest X-ray if CAP is suspected and the diagnosis is uncertain, symptoms are significant, or hospital assessment is needed
- Blood tests: FBC, U&E, CRP, LFTs as clinically indicated in secondary care
- Blood cultures in moderate/high severity CAP or if sepsis is suspected
- Sputum culture if productive cough and moderate/high severity disease or failure to improve
- Urinary antigen testing for pneumococcus or Legionella may be useful in selected admitted patients, especially severe CAP
- Viral testing may be appropriate depending on season, outbreak setting, or severity
- CT chest is not routine, but may be helpful if complications, malignancy, empyema, or alternative diagnoses are suspected
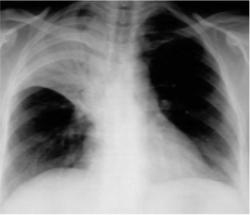
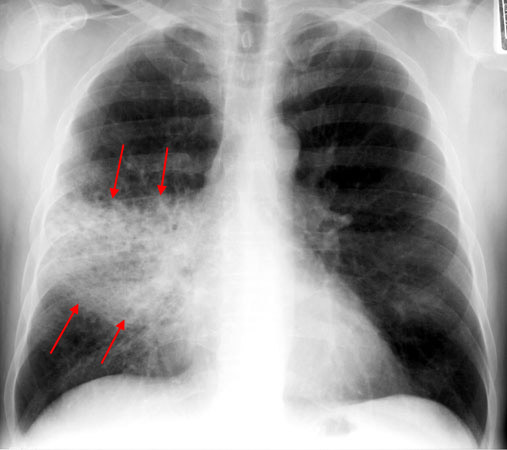
🖼️ Imaging
- Lobar consolidation suggests classical bacterial CAP, especially pneumococcal disease.
- Patchy or multilobar shadowing may occur in bronchopneumonia or severe disease.
- Interstitial or ground-glass change may suggest viral or atypical infection, but imaging patterns are not fully specific.
- Pleural effusion, cavitation, or non-resolving shadowing should prompt further review.
💊 Management
- Start antibiotics as soon as possible after diagnosis; in hospital this should be within 4 hours of presentation.
- Choose antibiotic according to severity, allergy status, local antimicrobial guidance, recent antibiotic exposure, and risk factors for resistant or unusual pathogens.
- Give oxygen if hypoxic, aiming for appropriate oxygen targets.
- Provide fluids, analgesia, antipyretics, and venous thromboembolism prophylaxis where indicated.
- Review for sepsis and escalate care early if deteriorating.
- If IV antibiotics are started, review regularly and switch to oral treatment when clinically appropriate.
- For adults with CAP, stop antibiotics after 5 days unless microbiology suggests otherwise or the person is not clinically stable.
💊 ITU Discussions in HAP
- Early senior review discuss with ITU if deteriorating despite initial treatment or has severe physiological derangement.
- Severe hypoxia escalating oxygen requirement, need for high-flow oxygen, CPAP/NIV or possible invasive ventilation.
- Septic shock persistent hypotension, rising lactate, poor peripheral perfusion or need for vasopressors despite fluid resuscitation.
- Respiratory fatigue rising respiratory rate, exhaustion, reduced consciousness or worsening hypercapnia/acidosis.
- Multi-organ dysfunction — acute kidney injury, coagulopathy, liver dysfunction, delirium, oliguria or worsening metabolic acidosis.
- High-risk host factors frailty, immunosuppression, major comorbidity, recent surgery, aspiration risk or poor physiological reserve.
- Source/control issues consider empyema, abscess, obstructing tumour, infected line or inadequate antimicrobial cover if not improving.
- Ceiling of care clarify escalation status, DNACPR, patient wishes, frailty score, reversibility and likely benefit of organ support.
💊 Community-Acquired Pneumonia (CAP) – Follow Local Antibiotic Guidance
Start antibiotics as soon as possible after diagnosis. In adults presenting to hospital, give antibiotics within 4 hours of presentation. For most adults with CAP, stop antibiotics after 5 days unless microbiology suggests a longer course or the patient is not clinically stable.
| Severity | First-line | If penicillin allergy / unsuitable | Notes |
|---|---|---|---|
| Low-severity CAP | Amoxicillin 500 mg PO three times daily for 5 days |
Doxycycline 200 mg PO on day 1, then 100 mg PO once daily for 4 more days
OR Clarithromycin 500 mg PO twice daily for 5 days OR Erythromycin 500 mg PO four times daily for 5 days (preferred macrolide in pregnancy) |
Higher doses of amoxicillin may be used in severe infection - check BNF/local policy. |
| Moderate-severity CAP | Amoxicillin 500 mg PO three times daily for 5 days PLUS if atypical pathogens suspected: Clarithromycin 500 mg PO twice daily for 5 days OR Erythromycin 500 mg PO four times daily for 5 days (if pregnant) | Doxycycline 200 mg PO on day 1, then 100 mg PO once daily for 4 more days OR Clarithromycin 500 mg PO twice daily for 5 days | Moderate-severity CAP often needs admission or close supervision. |
| High-severity CAP | Follow local hospital antimicrobial guideline urgently | Follow local hospital antimicrobial guideline urgently | Severe CAP usually requires IV antibiotics, broader cover, senior review, and sepsis / critical care assessment. |
🩺 Practical prescribing notes
- Use CURB-65 with clinical judgement to assess severity.
- Review IV antibiotics early and switch to oral when clinically appropriate.
- Check renal function, allergy history, pregnancy status, and drug interactions.
- Consider local resistance patterns, recent antibiotic exposure, aspiration risk, and risk of unusual pathogens.
- Do not keep antibiotics going automatically beyond 5 days without a reason.
💡 Do not hard-code antibiotic regimens without checking local antimicrobial policy. NICE gives the framework for timing, duration, review, and route, but hospitals usually specify exact antibiotic combinations locally.
⚠️ Complications
- Pleural effusion and empyema
- Lung abscess or necrotising pneumonia
- Sepsis and septic shock
- Respiratory failure
- ARDS
- Bronchiectatic damage after severe infection
- Delirium, falls, and deconditioning in older adults
🏥 When to seek senior / ICU input
- Increasing oxygen requirement or worsening work of breathing
- Hypotension or sepsis despite fluids
- Confusion, exhaustion, rising CO₂, or worsening acidosis
- Multilobar disease, rapidly progressive infiltrates, or respiratory failure
- Need for ventilatory support or vasopressors
🔁 Follow-up
- Clinical review is important if symptoms worsen or fail to improve as expected.
- Consider repeat chest X-ray, especially if symptoms persist, recovery is incomplete, or underlying malignancy is a concern.
- People who smoke, older adults, and those with persistent focal change may need follow-up imaging to ensure resolution.
🛡️ Prevention
- Smoking cessation Influenza vaccination and pneumococcal vaccination where indicated
- Optimise management of chronic lung disease and swallowing risk
- Reduce alcohol excess and frailty-related aspiration risk
📚 References
- NICE NG250: Pneumonia – diagnosis and management
- NICE NG250 recommendations
- NICE visual summary – CAP in adults presenting to primary care
- NICE visual summary – CAP in adults presenting to hospital
- BNF: Amoxicillin
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery