Related Subjects:
|Neurological History taking
|Causes of Stroke
|Ischaemic Stroke
|Subarachnoid Haemorrhage
|Cerebral Arterial Perfusion and Clinical Correlates
|Anterior circulation Brain
|Posterior circulation Brain
|Acute Stroke Assessment (ROSIER&NIHSS)
|Carotid Artery dissection
|Vertebral artery dissection
|Acute Stroke Assessment (ROSIER&NIHSS)
|Atrial Fibrillation
|Atrial Myxoma
|Causes of Stroke
|Ischaemic Stroke
|Cancer and Stroke
|Cerebral Venous thrombosis
|Cardioembolic stroke
|CT Basics for Stroke
|Endocarditis and Stroke
|Haemorrhagic Stroke
|Stroke Thrombolysis
|Hyperacute Stroke Care
|AP of the Brain
|Cryptogenic stroke
|Carotid Web
|Anterior / Medial Medullary Infarct (Dejerine Syndrome)
📖 About
- Always consider vertebral artery dissection in a young patient with posterior circulation stroke (esp. dizziness, ataxia, vision loss).
- Accounts for ~10–25% of strokes in young adults (<50 years).
- Pathology: vessel wall tear → intramural haematoma → luminal narrowing/thrombosis → emboli.
⚙️ Aetiology
- Dissection → intraluminal clot → embolisation or local occlusion.
- Common sites: at C1–C2 level or origin of the PICA.
- Connective tissue disorders (Ehlers–Danlos IV, fibromuscular dysplasia) predispose.
- Triggered by minor trauma or sudden neck movements (e.g. chiropractor, hairdresser basin, yoga, sports).
- Rare but severe: basilar artery dissection → high mortality.
🧬 Predisposing Factors
- 🦴 Neck trauma (rotation/flexion stresses).
- 🧬 Connective tissue disorders: Ehlers–Danlos IV, fibromuscular dysplasia, cystic medial necrosis.
- ⚡ Genetic conditions: Marfan, COL1 mutations, osteogenesis imperfecta type 1.
- 🧠 Migraine, family history of dissection.
- 🚺 Pregnancy and postpartum state.
- 🚬 Smoking as an acquired risk factor.
Normal Angiography with carotids removed
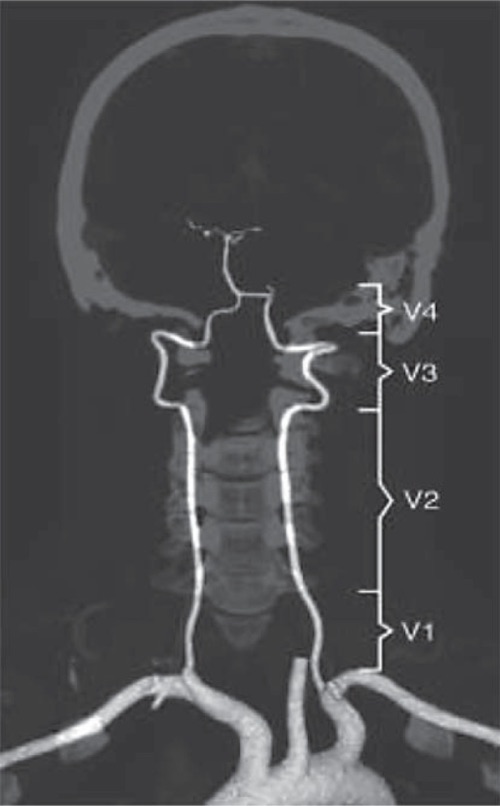
Left Proximal Vertebral dissection

🩺 Clinical Presentation
- 🪖 Headache/neck pain (often sudden, occipital, unilateral).
- 🎯 Posterior circulation stroke signs: dizziness, diplopia, vertigo, dysarthria, ataxia.
- 🧑⚕️ Lateral medullary (Wallenberg) syndrome: ipsilateral facial numbness, contralateral body numbness, dysphagia, hoarseness, Horner’s syndrome.
- 💢 Intracranial dissections: may rupture → subarachnoid haemorrhage (SAH) (up to 50% cases).
🔍 Investigations
- 🖼️ CTA: Best initial test – shows vessel narrowing, occlusion, or dissection flap.
- 🧲 MRI/MRA with fat suppression: Characteristic crescent sign = intramural haematoma.
- 📡 Doppler ultrasound: May suggest occlusion or flow turbulence, but less sensitive in vertebral arteries.
⚖️ Management
- 💊 Anticoagulation (warfarin) for 3–6 months was traditional; evidence is mixed.
- 💊 Dual antiplatelet therapy (aspirin + clopidogrel) is now often used as an alternative, esp. if SAH risk.
- 📉 Choice of antithrombotic depends on location:
– Extracranial dissection → antithrombotic therapy reasonable.
– Intracranial dissection → higher SAH risk → anticoagulation often avoided.
- 🧑⚕️ Basilar dissections: poor prognosis, sometimes considered for stenting but evidence limited.
- 📆 Follow-up vascular imaging at 3–6 months to assess healing.
💡 Exam Pearls:
– Think vertebral dissection in a young patient with posterior circulation stroke + neck pain.
– Crescent sign on MRI is classic.
– Management: antithrombotics (antiplatelet or anticoagulation) but intracranial dissections carry SAH risk.
