🔗 Related Subjects:
| 💪 Myasthenia Gravis
| ⚡ Lambert-Eaton syndrome (LEMS)
|Motor Neuron Disease (MND-ALS)
|Miller-Fisher syndrome
|Guillain Barre Syndrome
|Multifocal Motor Neuropathy with Conduction block
|Multiple Sclerosis (MS) Demyelination
😴 Myasthenia gravis (MG) causes fluctuating, fatigable weakness of ocular, bulbar, respiratory, neck and limb muscles.
🧠 Sensation and reflexes are usually normal. Symptoms often worsen with repeated use and improve with rest.
🚑 Myasthenic Crisis — Practical Treatment
- Admit to ICU/HDU if respiratory, bulbar or rapidly progressive weakness.
- Monitor FVC, respiratory effort, cough strength, swallowing and secretion control.
- Treat infection, aspiration, electrolyte disturbance and medication triggers.
- Use IVIg or plasma exchange urgently for significant crisis.
- Consider temporarily withholding pyridostigmine if intubated or if secretions are problematic; restart with neurology advice.
- Avoid sedatives, magnesium and neuromuscular blockers unless essential and specialist-supervised.
📖 About
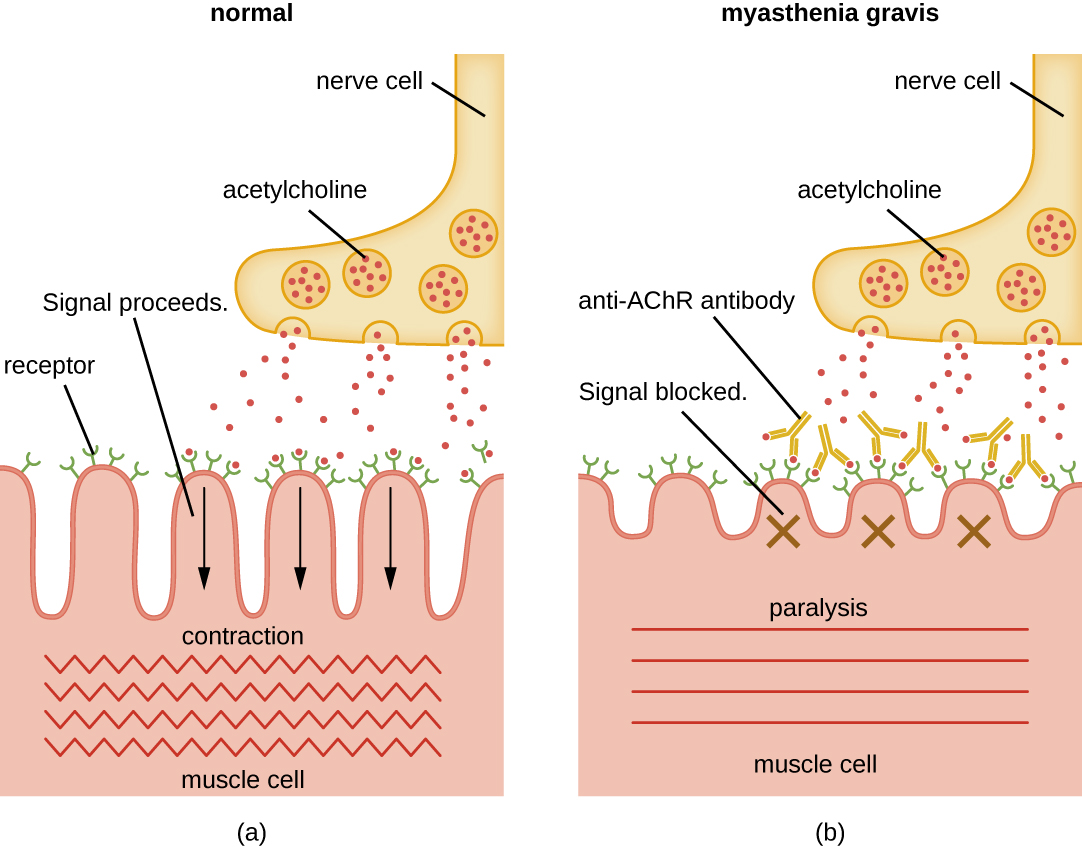
- 🧬 MG is an autoimmune disorder of the neuromuscular junction.
- Autoantibodies reduce effective neuromuscular transmission, most commonly by targeting the acetylcholine receptor.
- The hallmark is fatigable weakness: repeated activity worsens power, while rest may improve it.
- Weakness commonly affects ocular, facial, bulbar, neck flexor, proximal limb and respiratory muscles.
- Pupils, sensation and tendon reflexes are usually normal.
🧪 Aetiology / Antibodies
| Antibody |
Clinical relevance |
| Anti-AChR |
- Most common antibody in MG.
- Present in about 80–85% of generalised MG, but less sensitive in purely ocular MG.
- Associated with thymic hyperplasia and thymoma.
|
| Anti-MuSK |
- Seen in a proportion of AChR-negative generalised MG.
- Often associated with prominent bulbar, facial, neck or respiratory weakness.
- May respond less well to pyridostigmine and may need specialist immunotherapy.
|
| Anti-LRP4 |
- low-density lipoprotein receptor-related protein 4
- Uncommon; may be found in some “double-seronegative” MG.
- Testing availability varies.
|
| Anti-titin / anti-RyR |
- Striational antibodies.
- May be associated with thymoma or late-onset MG.
- Usually specialist tests rather than first-line diagnostic tests.
|
| Seronegative MG |
- Negative antibodies do not exclude MG.
- Diagnosis may require neurophysiology, especially single-fibre EMG.
|
🧨 Pathophysiology
- Anti-AChR antibodies cause complement-mediated damage to the postsynaptic membrane.
- There are fewer functioning acetylcholine receptors and simplified postsynaptic folds.
- The “safety margin” for neuromuscular transmission falls.
- With repeated stimulation, acetylcholine release normally declines slightly; in MG this produces transmission failure and fatigable weakness.
🔗 Clinical Associations
- 🦋 Autoimmune disease: thyroid disease, rheumatoid arthritis, SLE, Sjögren’s disease.
- 🩸 Pernicious anaemia.
- 🧬 Thymic hyperplasia or thymoma.
- 🧩 Other autoimmune conditions may coexist, but thyroid disease is especially important to check.
🧩 Clinical Features
| System |
Features |
| Ocular |
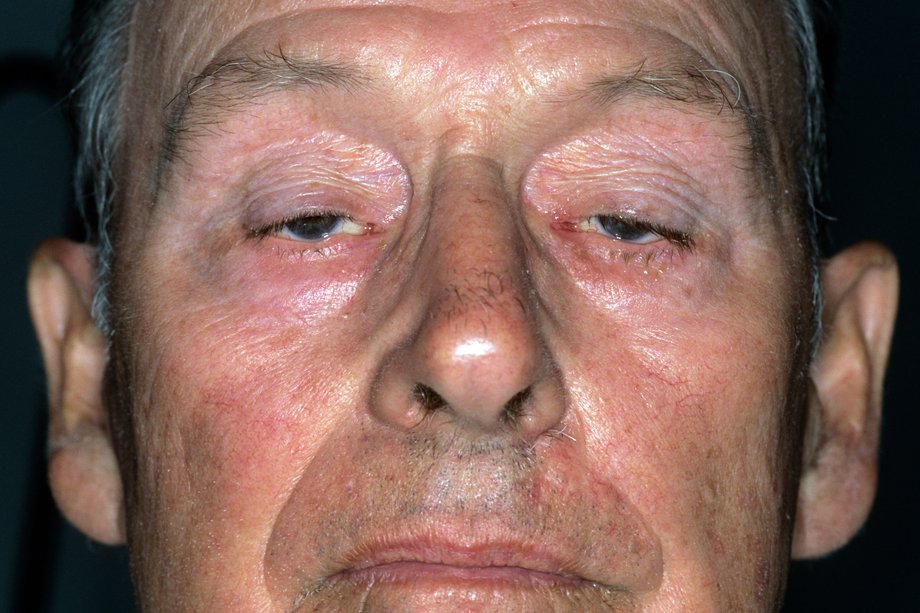
- 👀 Fluctuating ptosis and diplopia.
- 👁️ Pupils are spared.
- 🧊 Ice-pack test may improve ptosis.
- 👁️ Cogan’s lid twitch may be seen.
|
| Bulbar |
- 🍽️ Dysphagia, choking, nasal regurgitation.
- 🗣️ Dysarthria, nasal speech or voice fading with prolonged talking.
- 😬 Chewing fatigue and “myasthenic snarl”.
|
| Limb / axial |
- 💪 Fatigable proximal limb weakness.
- 🧍 Neck flexor weakness, head drop.
- ♻️ Symptoms worsen with repeated activity and later in the day.
|
| Respiratory |
- 🫁 Dyspnoea, weak cough, orthopnoea or inability to clear secretions.
- ⚠️ Myasthenic crisis may cause life-threatening ventilatory failure.
|
| Pregnancy |
- 🤰 Symptoms may worsen in pregnancy or postpartum.
- 👶 Transient neonatal MG can occur due to passive antibody transfer.
|
🧾 Differential Diagnosis
- ⚡ Lambert-Eaton myasthenic syndrome — proximal weakness, autonomic symptoms, reflexes improve after exercise; associated with small-cell lung cancer.
- ☠️ Botulism — pupils often affected, autonomic features, descending paralysis.
- 💊 Drug-induced worsening — aminoglycosides, fluoroquinolones, magnesium, beta-blockers and others.
- 🧿 Chronic progressive external ophthalmoplegia.
- 🧠 Brainstem stroke, multiple sclerosis, motor neurone disease or mitochondrial disease depending on presentation.
- 🦋 Thyroid eye disease if ocular symptoms predominate.
🔎 Investigations
- 🧪 Anti-AChR antibody first-line.
- 🧪 Anti-MuSK antibody if AChR negative and suspicion remains.
- 🧪 Consider LRP4 or specialist antibody testing if AChR/MuSK negative.
- ⚡ Neurophysiology: repetitive nerve stimulation shows decrement; single-fibre EMG is highly sensitive.
- 🧊 Ice-pack test may support ocular MG with ptosis.
- 🫁 Respiratory function: FVC and negative inspiratory force in suspected crisis.
- 🫀 CT or MRI chest to assess thymus / thymoma once MG is confirmed or strongly suspected.
- 🦋 TFTs to check for thyroid disease.
- 🚫 Edrophonium/Tensilon test is historical and not routinely used in modern UK practice.
⚡ Neurophysiology in Myasthenia Gravis
| Test |
Finding |
Meaning |
| Repetitive nerve stimulation |
Decremental response |
With repeated stimulation, the compound muscle action potential progressively falls because neuromuscular transmission fails.
|
| Single-fibre EMG |
Increased jitter |
Jitter is the variation in timing between action potentials from two muscle fibres supplied by the same motor axon. Increased jitter indicates unstable neuromuscular transmission.
|
| Single-fibre EMG |
Blocking |
In more severe transmission failure, some impulses fail to generate a muscle fibre action potential at all.
|
📌 Learning tip: In MG, repetitive nerve stimulation shows decrement; single-fibre EMG shows increased jitter.
SFEMG is very sensitive, but not perfectly specific, so results must be interpreted with the clinical picture and antibody testing.
❓ Key Diagnostic Questions
- Is this ocular MG or generalised MG?
- Are there bulbar or respiratory symptoms suggesting impending crisis?
- Is the patient AChR-positive, MuSK-positive, LRP4-positive or seronegative?
- Is there thymoma or thymic hyperplasia?
- Could this be Lambert-Eaton, botulism, thyroid eye disease or a brainstem disorder?
- Is a medication or infection worsening the weakness?
🚫 Drugs That May Worsen MG
| Drug / class |
Comment |
| 💊 Aminoglycosides e.g. gentamicin |
Can impair neuromuscular transmission and precipitate severe weakness. |
| 💊 Fluoroquinolones e.g. ciprofloxacin, levofloxacin |
Use cautiously, if at all, because worsening MG has been reported. |
| 💊 Macrolides e.g. erythromycin, azithromycin |
May worsen weakness in susceptible patients. |
| 💊 Telithromycin |
Should be avoided; strongly associated with severe MG exacerbation. |
| 💊 Magnesium |
Can worsen neuromuscular transmission; avoid IV magnesium unless essential and specialist-supervised. |
| 💊 Beta-blockers |
May worsen weakness; use caution and monitor. |
| 💊 Phenytoin, quinidine, procainamide |
May impair neuromuscular transmission. |
| 💊 Botulinum toxin |
Avoid or use only with specialist advice. |
| 💊 D-penicillamine |
Can induce MG by triggering AChR antibodies. |
| 💊 Neuromuscular blockers |
High risk of prolonged weakness; anaesthetic team must be aware of MG. |
🛠️ Management
🚨 Myasthenic Crisis — Initial Management
| Feature |
Action |
| Red flags |
- 🫁 Dyspnoea, shallow breathing, exhaustion, weak cough or inability to count aloud.
- 😮 Dysphagia, choking, nasal speech, dysarthria or pooling secretions.
- ⚠️ Cyanosis, aspiration, pneumonia, sepsis or rapidly worsening weakness.
- 📉 Low or falling forced vital capacity / negative inspiratory force where measured.
|
| Immediate approach |
- 🚑 ABCDE, Give oxygen, senior review and early ICU/anaesthetic involvement.
- 🫁 Assess resp function repeatedly. Check ABG/VBG, FVC if possible. O2 sats fall late. Intubate early if needed.
- 🧪 Check Glucose, U&Es, infection markers and CXR if infection/aspiration suspected.
- 💊 Review and stop drugs that may worsen MG where possible. Avoid Gentamicin
|
| Disease-specific treatment |
- 🩸 Use IV immunoglobulin or plasma exchange for significant crisis or rapidly progressive weakness.
- 🦠 Treat triggers: infection, aspiration, surgery, pregnancy/postpartum, medication change or poor adherence.
- ⚠️ Pyridostigmine may be temporarily withheld in intubated patients or those with excessive secretions; restart under specialist guidance.
- 🧠 Involve neurology early for longer-term immunotherapy planning.
|
| Important caveat |
- ⚖️ Distinguish myasthenic crisis from cholinergic excess, although true cholinergic crisis is now uncommon.
- 💦 Cholinergic excess may cause salivation, sweating, diarrhoea, abdominal cramps, bradycardia, fasciculations and worsening weakness.
- 🚫 Edrophonium/Tensilon testing is not routine and should not delay ventilatory support or specialist treatment.
|
| Treatment |
Role |
Notes |
| Pyridostigmine |
Symptomatic treatment |
Often started at low dose and titrated. Useful for ocular and generalised symptoms, but may be less helpful or less tolerated in MuSK-positive disease. |
| Prednisolone |
Immunosuppression / disease control |
Usually introduced carefully because steroids can initially worsen MG. Recent ABN guidance emphasises daily steroid regimens as standard practice. |
| Steroid-sparing immunosuppressants |
Long-term disease control |
Azathioprine, mycophenolate, ciclosporin, tacrolimus or methotrexate may be used under specialist care. |
| IVIg or plasma exchange |
Rapid short-term improvement |
Used for myasthenic crisis, severe bulbar/respiratory weakness, pre-operative optimisation or severe exacerbations. |
| Rituximab |
Refractory disease |
Particularly considered in refractory MuSK-positive MG under specialist neurology care. |
| Rozanolixizumab |
Selected refractory antibody-positive generalised MG |
NICE-recommended for some adults with antibody-positive generalised MG not controlled by existing treatment. |
| Thymectomy |
Thymoma and selected generalised AChR-positive MG |
Indicated for thymoma. Also considered early in appropriate AChR-positive generalised MG to improve long-term disease control. |
| Pregnancy |
Specialist management |
Pyridostigmine is generally considered safe. Steroids may be used if required. Avoid teratogenic immunosuppressants and involve neurology/obstetrics early. |
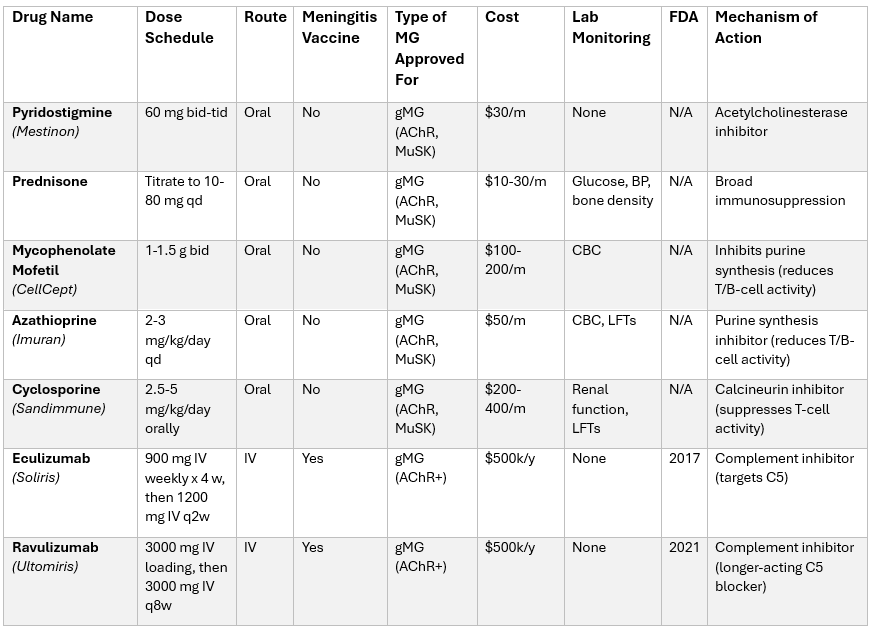
💊 Medications in MG
📚 References
Cases - Myasthenia Gravis (MG)
- Case 1 - Ocular Myasthenia 👁️:
A 28-year-old woman reports drooping of her right eyelid that worsens by evening and double vision after prolonged reading. Examination shows fatigable ptosis and ophthalmoparesis, with normal pupils, sensation and reflexes.
Diagnosis: Ocular myasthenia gravis.
Management: Anti-AChR antibodies, consider MuSK if negative, neurophysiology if needed, pyridostigmine for symptoms, and monitor for progression to generalised MG.
- Case 2 - Generalised MG with Bulbar Symptoms 🗣️:
A 45-year-old man presents with fluctuating limb weakness, nasal speech and difficulty swallowing, especially late in the day. Examination shows fatigable proximal weakness, weak neck flexion and reduced palatal movement.
Diagnosis: Generalised MG with bulbar involvement.
Management: Neurology review, pyridostigmine, immunosuppression, swallowing assessment, screen for thymoma with CT chest and safety-net for respiratory deterioration.
- Case 3 - Myasthenic Crisis in ICU ⚠️:
A 52-year-old woman with known MG develops pneumonia and acute worsening weakness, now with difficulty speaking and shallow breathing. Examination shows weak cough and reduced vital capacity.
Diagnosis: Myasthenic crisis precipitated by infection.
Management: ICU/anaesthetic review, ventilatory support if required, IVIg or plasma exchange, treat pneumonia, avoid MG-worsening drugs and optimise long-term immunotherapy.
Teaching Commentary 🧠
Myasthenia gravis is an autoimmune disorder of the neuromuscular junction, usually due to antibodies against AChR or MuSK.
The clinical hallmark is fluctuating, fatigable weakness, especially ocular, bulbar, neck, proximal limb and respiratory weakness, with normal sensation and reflexes.
AChR antibodies are the first-line test, but negative antibodies do not exclude MG; MuSK, LRP4 and neurophysiology may be needed.
The dangerous presentation is myasthenic crisis, where bulbar and respiratory weakness can progress to ventilatory failure even before oxygen saturations fall.
Treatment includes pyridostigmine for symptoms, immunotherapy for disease control, IVIg or plasma exchange for crisis, and thymectomy for thymoma or selected AChR-positive generalised disease.
```
