
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Chronic Myeloid Leukaemia (CML) ✅
Related Subjects: |Leukaemias in General |Acute Promyelocytic Leukaemia |Acute Myeloblastic Leukaemia (AML) |Acute Lymphoblastic Leukaemia (ALL) |Chronic Lymphocytic leukaemia (CLL) |Chronic Myeloid Leukaemia (CML) |Hairy Cell Leukaemia |Differentiation syndrome |Tretinoin (All-trans-retinoic acid (ATRA) ) |Haemolytic anaemia |Immune(Idiopathic) Thrombocytopenic Purpura (ITP) |Polycythaemia Vera (Primary Polycythaemia)
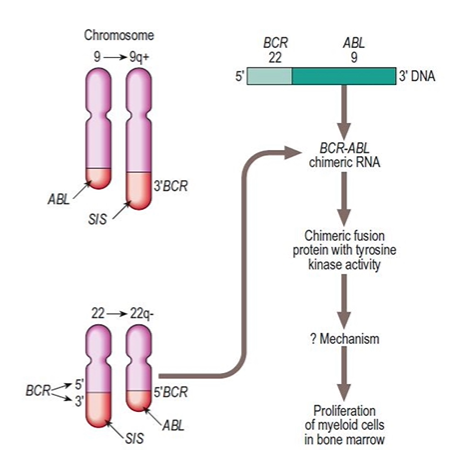
The BCR-ABL fusion protein (p210 BCR-ABL1) is the product of the Philadelphia chromosome t(9;22), found in the vast majority of cases of Chronic Myeloid Leukaemia (CML). It is a constitutively active tyrosine kinase that stimulates uncontrolled signal transduction, proliferation and inhibits apoptosis. Tyrosine kinase inhibitors (TKIs) such as imatinib, dasatinib and nilotinib are first-line treatment options for the chronic phase of CML (NICE TA426).
ℹ️ About
- A myeloproliferative stem cell disorder predominantly involving granulocytes.
- Typically seen in patients aged 40-75 years (median age around 65).
🧬 Aetiology
- Cytogenetic analysis reveals the t(9;22) Philadelphia chromosome in >95% of cases.
- This forms the BCR-ABL fusion gene, which codes for a 210 kDa protein.
- The BCR-ABL protein has constitutive tyrosine kinase activity, acting as an oncogene.
Stages of CML
- Chronic phase: Can last up to 5 years untreated; often indefinitely prolonged with effective TKI treatment. Most patients present in this phase.
- Accelerated phase: A more aggressive phase that may develop after the chronic phase (defined by specific criteria such as 10-19% blasts).
- Blast crisis: CML can progress to either Acute Myeloid Leukaemia (AML) or Acute Lymphoblastic Leukaemia (ALL). This phase is more difficult to treat and has become less frequent with early TKI therapy.
🩺 Clinical Features
- Many patients are asymptomatic at diagnosis (incidental leukocytosis on routine FBC).
- When symptomatic: fever, night sweats, weight loss (B symptoms), and occasionally priapism.
- Abdominal pain or peptic ulcer disease (due to histamine release from increased basophil cell mass).
- Massive splenomegaly, which may cause acute abdominal pain from splenic infarction.
- Lymphadenopathy is uncommon, except during blast crisis.
- CML may progress to AML or myelofibrosis over time if untreated.
- Bone marrow failure can occur in later stages.
🔎 Investigations
- Full Blood Count (FBC): WCC may exceed 50-400 x 10⁹/L, with left shift (predominantly neutrophils, myelocytes, and metamyelocytes). High platelet counts may also be observed. Basophilia common.
- BCR-ABL1: Detected by FISH, cytogenetics or reverse transcriptase PCR (Philadelphia chromosome).
- Leukocyte Alkaline Phosphatase (LAP) score: Low in CML (helps differentiate from reactive leukocytosis).
- Bone Marrow: Hypercellular, with greatly increased granulocytic production.
- Lactate Dehydrogenase (LDH): Elevated in CML due to increased cell turnover.
- Uric Acid Levels: Elevated due to increased cell breakdown.
Prognosis: depends on several factors
- Age at diagnosis.
- Phase of CML at the time of diagnosis.
- Number of blasts in the blood and bone marrow.
- Size of the spleen at diagnosis.
- General health of the patient and risk score (e.g. ELTS/Sokal).
💊 Management
- Tyrosine Kinase Inhibitors (TKIs): The mainstay of treatment. NICE TA426 recommends imatinib, dasatinib or nilotinib for untreated chronic-phase Philadelphia chromosome-positive CML in adults. These achieve high rates of hematologic and cytogenetic response, with excellent long-term survival in the chronic phase (often >90%).
- Imatinib: Blocks the action of the BCR-ABL fusion protein. Leads to complete cytogenetic response (disappearance of the Philadelphia chromosome) in the majority of patients over time.
- Patients are monitored by quantitative PCR for BCR-ABL1 transcript levels (on International Scale) to assess treatment response. Optimal response at 3 months is BCR-ABL1 ≤10%. Some patients develop resistance (often due to ABL kinase domain mutations), requiring switch to alternative (2nd/3rd generation) TKIs.
- Allogeneic Hematopoietic Stem Cell Transplant (HSCT): Reserved for patients who fail multiple TKIs, have T315I mutation, or present with advanced phase disease.
- Blast Crisis: Combination of TKI and intensive chemotherapy is given; allogeneic HSCT is often considered if response achieved.
- Supportive/Palliative Treatments: Hydroxycarbamide (hydroxyurea) for initial cytoreduction in symptomatic patients or high WCC, and in palliative settings for older/unfit patients. Low-dose cytarabine rarely used now.
NICE References: TA426 (Dasatinib, nilotinib and imatinib for untreated chronic myeloid leukaemia, 2016 – active); TA70 (Imatinib for chronic myeloid leukaemia, 2003 – partially superseded by TA426). For newer agents (e.g., asciminib after ≥2 TKIs), see TA813.
Cases - Chronic Myeloid Leukaemia (CML)
- Case 1 - Incidental Leukocytosis:
A 55-year-old man has a routine FBC for a pre-op check. WCC is 45 ×10⁹/L, Hb 13.6 g/dL, platelets 420 ×10⁹/L. He is asymptomatic. Blood film shows myelocytes, metamyelocytes, and basophilia. BCR-ABL fusion gene is detected. Diagnosis: CML in chronic phase. - Case 2 - Symptomatic Splenomegaly:
A 48-year-old woman presents with early satiety, weight loss, and night sweats. Examination reveals massive splenomegaly extending to the iliac fossa. Bloods: WCC 110 ×10⁹/L, Hb 10.2 g/dL, platelets 650 ×10⁹/L. Bone marrow aspirate shows hypercellularity with granulocytic proliferation. Diagnosis: CML, accelerated phase. - Case 3 - Transformation (“Blast Crisis”):
A 60-year-old man with known CML presents with fever, bone pain, and bruising. FBC shows WCC 80 ×10⁹/L with 35% blasts, Hb 7.4 g/dL, platelets 45 ×10⁹/L. He has pancytopenia and is acutely unwell. Diagnosis: CML in blast crisis (resembles acute leukaemia).
Teaching Commentary 🧬
CML is a myeloproliferative neoplasm driven by the Philadelphia chromosome (t(9;22)) producing the BCR-ABL1 tyrosine kinase, which promotes uncontrolled myeloid proliferation. The disease classically progresses through chronic, accelerated, and blast crisis phases if untreated. Splenomegaly and systemic “B symptoms” are common features. Modern management has been revolutionised by tyrosine kinase inhibitors (TKIs) such as imatinib, dasatinib and nilotinib, which can induce long-term remission and near-normal life expectancy in chronic phase. Monitoring is via qPCR for BCR-ABL1 transcript levels. Allogeneic stem cell transplantation is now reserved for TKI-resistant or advanced disease. (NICE TA426)