
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Primary amoebic meningoencephalitis (PAM)
🧠 Naegleria fowleri (“brain-eating amoeba”) is rare but almost universally fatal. Most infections occur in young males, especially ≤14 years old. Mortality exceeds 95%, making early recognition and prevention critical.
🌍 About
- Causes a rapidly progressive brain infection in children and adolescents.
- Leads to severe cerebral swelling and herniation.
- Less common in chlorinated or salt water (chlorination protective).
🦠 Aetiology
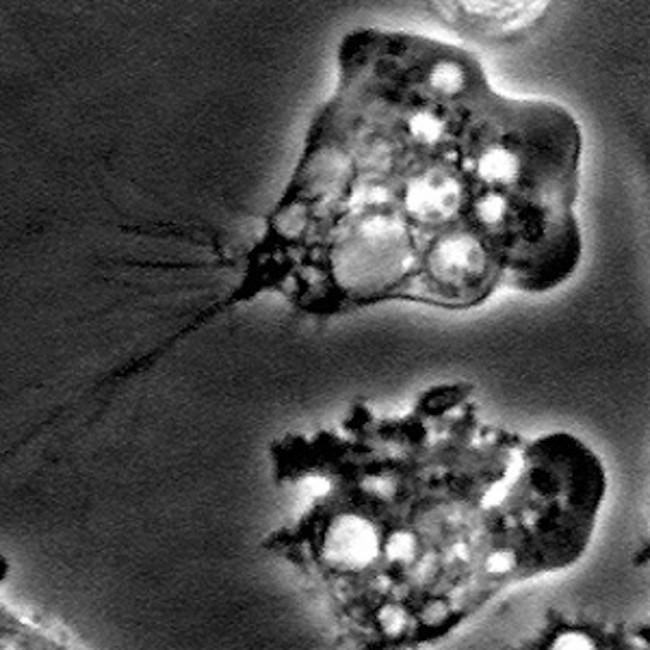
- Naegleria fowleri – a free-living thermophilic amoeba.
- Found in warm fresh water 💧 (lakes, rivers, hot springs) and soil.
- Risk in unchlorinated swimming pools 🏊♂️.
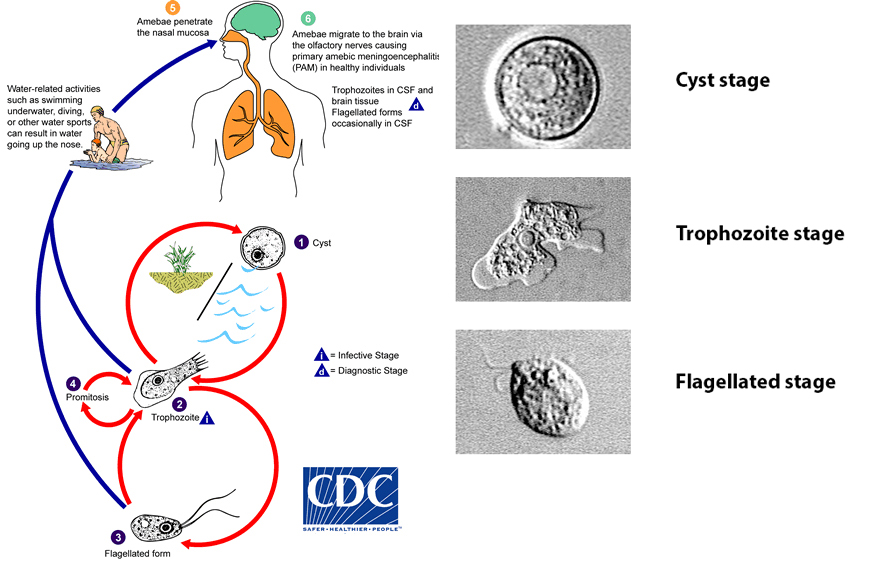
- Enters via the nose → olfactory nerves → cribriform plate → brain.
- Usually linked to swimming, diving, or water sports with head submersion.
⚠️ Clinical
- Onset usually within 1 week of exposure.
- Initial: headache, fever, nausea, vomiting 🤒.
- Meningism: stiff neck, photophobia, confusion.
- Progression: seizures, hallucinations, coma → death.
🔎 Investigations
- FBC, U&E, LFTs: usually unremarkable.
- CT/MRI: cerebral swelling, oedema, haemorrhage.
- CSF (if safe): often grey–red, high RBCs, neutrophilic pleocytosis (>28,000 WCC), ↑ protein, trophozoites may be seen on wet mount. 🚨 Often avoided due to raised ICP.
💊 Management
- Mortality >95%; only ~10 documented survivors worldwide 🌍.
- Supportive: ABC, resuscitation, ICP management.
- Often misdiagnosed and treated empirically as bacterial meningitis.
- Antimicrobials tried: Amphotericin B (IV + intrathecal), Azithromycin, Fluconazole, Rifampin, Miltefosine, Dexamethasone.
- Early aggressive combination therapy + ICP management offers the best (but still slim) chance of survival.
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery