Neurological Sensory Examination (OSCE)
Related Subjects:
|Neurological History taking
|Cortical functions
|Motor System
|Sensory System
|Mental State Examination
|Speech and Language Exam
|Cranial nerves and examination
|Assessing Cognition
🧠 Anatomy
- Conscious sensation travels from the receptor → spinal cord → thalamus → contralateral parietal lobe.
- Entry: via the dorsal root of the spinal cord.
- Two key ascending pathways:
- 🌟 Dorsal Columns: Proprioception, vibration, fine touch. Fibres ascend ipsilaterally → decussate in medulla → contralateral cortex.
- 🔥 Spinothalamic Tracts: Pain, temperature, crude touch. Fibres decussate almost immediately → ascend contralaterally → thalamus → cortex.
- Basic exam: Compare both sides with pinprick & cotton wool, test proprioception & temperature.
🔎 Sensory Modalities
- Proprioception (Dorsal Column): Move distal joints (finger/toe up/down) with eyes closed.
🌐 Romberg Test: Feet together, eyes closed. Instability = dorsal column dysfunction.
- Vibration (Dorsal Column): 128 Hz tuning fork on bony prominences (e.g. hallux, malleolus).
- Temperature (Spinothalamic): Use warm/cold tubes or tuning fork. Loss = spinothalamic lesion (e.g. Brown-Séquard, lateral medullary syndrome).
- Fine Touch (Dorsal Column): Cotton wool over dermatomes, moving from abnormal → normal.
- Pinprick (Spinothalamic): Disposable neurotip/pin for pain perception.
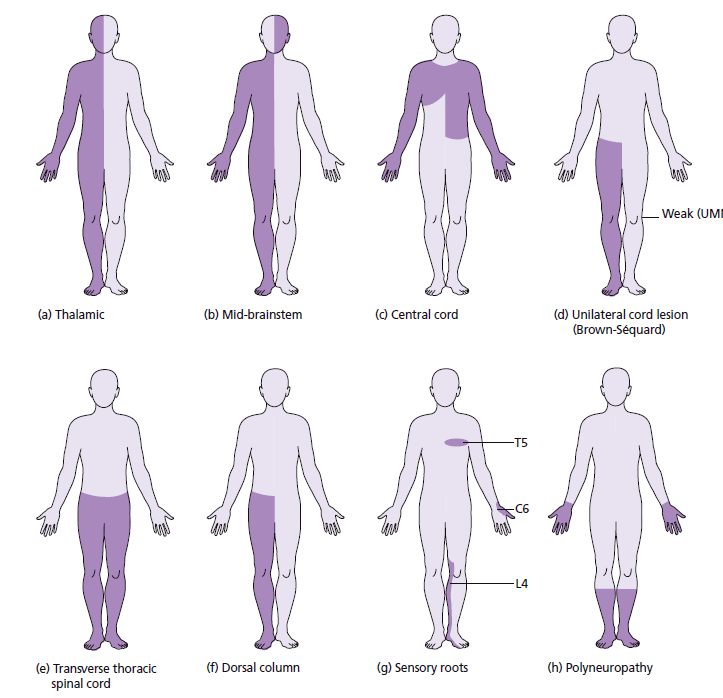
🩺 Interpretation
- 🧩 Patterns of sensory loss:
- Hemibody (face/arm/leg) → contralateral brain lesion.
- Cape-like loss over shoulders/arms → syringomyelia.
- Loss of vibration/proprioception → B12 deficiency (SACD, tabes dorsalis).
- Glove & stocking → peripheral neuropathy (e.g. diabetes).
- Sensory level → spinal cord lesion.
- Reduced perineal sensation → cauda equina syndrome.
- 🩺 Perineal exam: Essential if cauda equina suspected → check saddle sensation, anal tone, continence history.
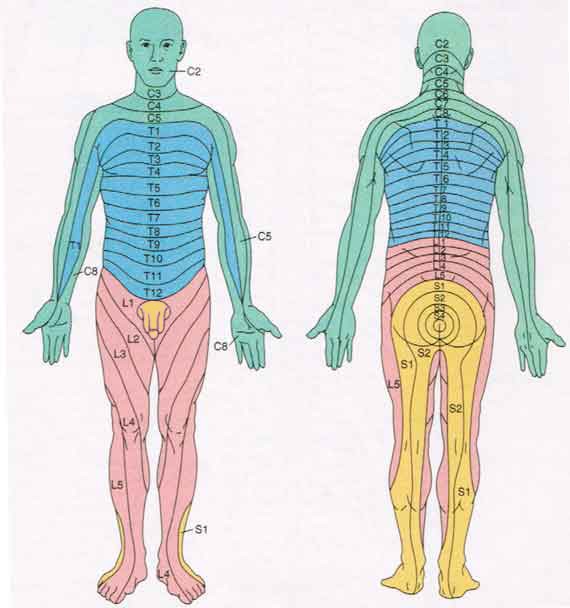
📍 Dermatomes
- 👍 Thumb: C6
- ☝️ Middle finger: C7
- 🤏 Little finger: C8
- 👕 Nipple line: T4
- 🪙 Umbilicus: T10
- 🦶 Big toe: L5
- 🦵 Little toe: S1
- 👖 Inner thigh: S2
- 🪑 Saddle area: S3–S5
🧾 Examination Steps (OSCE Style)
1. Introduction & Consent
- Introduce yourself, confirm patient identity & role.
- Explain procedure: “I’ll be testing different types of sensation.”
- Gain verbal consent, check comfort.
2. General Principles
- Position: patient seated or supine, relaxed.
- Exposure: only necessary areas, maintain dignity.
- Equipment: cotton wool, pin/neurotip, tuning fork (128 Hz), warm/cold tubes.
3. Light Touch
- Use cotton wool. Patient closes eyes, responds “yes” when touched.
- Compare both sides; map abnormalities.
4. Pain (Sharp/Dull)
- Use pin/neurotip alternating sharp vs blunt.
- Patient identifies “sharp” vs “dull.”
- Loss → spinothalamic dysfunction.
5. Temperature
- Use warm vs cold test tubes.
- Patient distinguishes warm vs cold → spinothalamic tract.
6. Vibration
- Strike tuning fork, place on bony prominence (toe, ankle, sternum).
- Ask patient when vibration starts/stops.
- Loss → peripheral neuropathy or dorsal column lesion.
7. Proprioception
- Hold digit by sides, move up/down with eyes closed.
- Patient identifies movement direction.
- Loss → dorsal column dysfunction.
8. Higher Discriminative Sensation
- Two-point discrimination: Paperclip/calipers.
- Graphesthesia: Draw number on palm.
- Stereognosis: Identify familiar object (coin, key) in hand.
