Cannonball Metastases
💣 Cannonball metastases = large, round, well-defined pulmonary metastases seen on CXR or CT.
They resemble “cannonballs” due to their spherical appearance.
🫁 Most often due to haematogenous spread of malignancy. Their discovery usually indicates advanced disease.
🎯 Common Primary Cancers Associated
- Renal Cell Carcinoma (RCC): Classic cause; often presents late with lung mets. 🟢
- Choriocarcinoma: Aggressive; spreads rapidly to lung, causing hemorrhagic cannonballs. 👩🍼
- Testicular Cancer (NSGCT): Young men may present with cannonball lesions on CXR. ⚽
- Prostate Cancer: Rare, usually very advanced disease. 🧔
- Breast Cancer: Can produce pulmonary metastases but less often “cannonball-like.” 🎀
- Sarcomas: Especially osteosarcoma & soft tissue sarcoma. 🦴
- Colorectal Cancer: Occasionally produces round pulmonary metastases. 🍽️
👀 Radiological Appearance

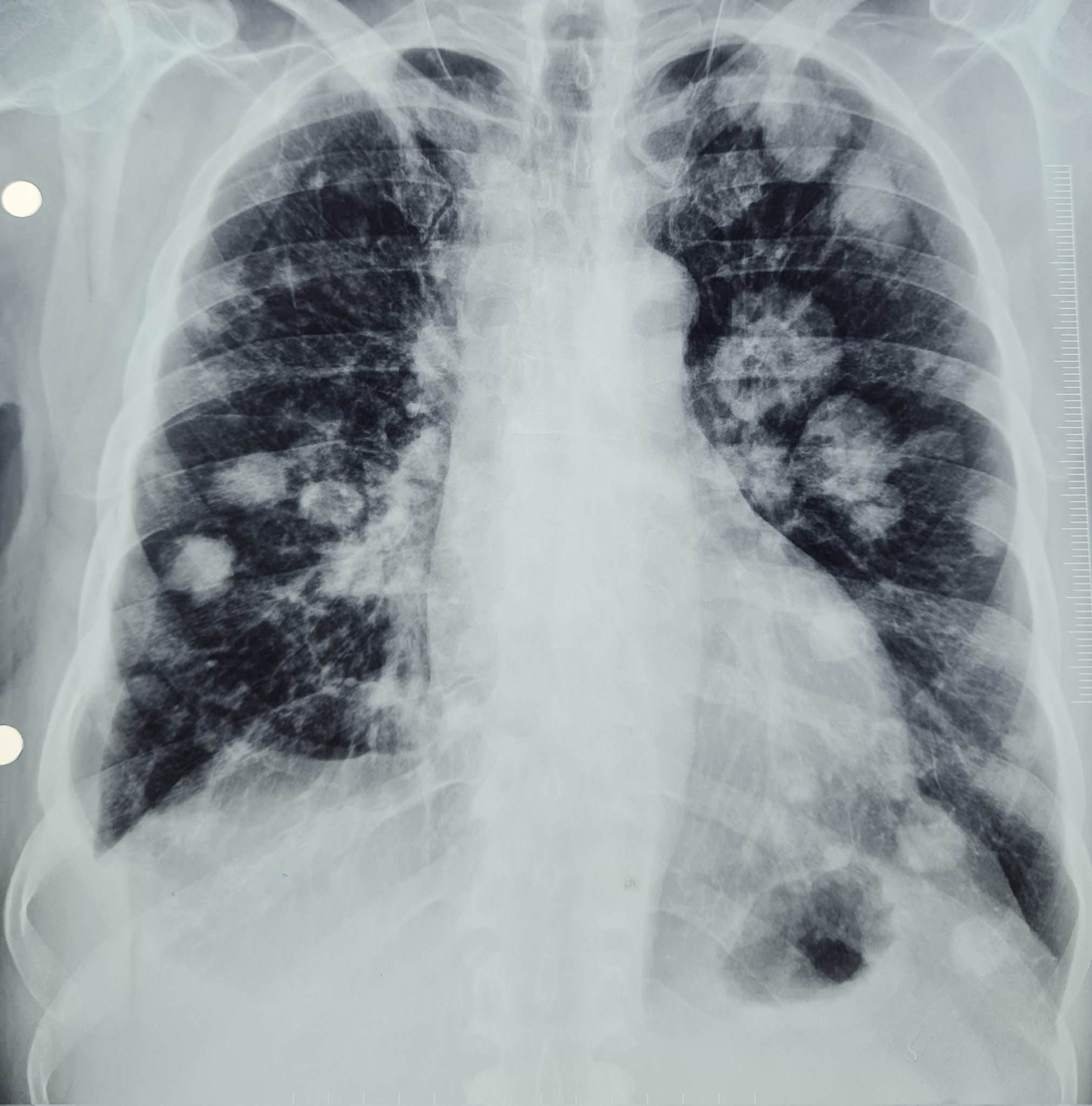
- Chest X-ray: Multiple, round, well-circumscribed opacities in both lungs ➝ “snowstorm” of nodules. 🌨️
- CT Scan: Precise size, number, distribution; assesses pleura & nodes. 🖥️
- Pattern: Bilateral, widespread, random distribution ➝ hallmark of haematogenous spread. 🌍
🩺 Clinical Presentation
- Often asymptomatic: Incidental finding during staging scans.
- Cough & Dyspnoea: From bulk disease or airway irritation. 😮💨
- Hemoptysis: Due to vascular invasion. 🚨
- B Symptoms: Weight loss, fever, night sweats, fatigue. ⚡
🔀 Differential Diagnosis
- Primary lung cancer (usually spiculated, not rounded).
- Granulomatous infection ➝ TB, fungal disease, sarcoid 🦠.
- Rheumatoid nodules (in seropositive RA). ✋
- Wegener’s (GPA) ➝ cavitating nodules. 🧩
- Septic emboli ➝ esp. IVDU or endocarditis. 💉
🧪 Diagnostic Workup
- Imaging: CXR ➝ CT chest ➝ PET-CT for staging.
- Biopsy: CT-guided or bronchoscopic biopsy for histology & IHC. 🔬
- Tumour Markers:
- β-hCG ➝ choriocarcinoma/testicular cancer.
- AFP ➝ germ cell tumours.
- PSA ➝ prostate cancer.
- Systemic staging: Abdomen/pelvis imaging for RCC, germ cell, colorectal. 🖥️
💊 Management
- Depends on primary tumour:
- RCC ➝ TKIs, immunotherapy (pembrolizumab, nivolumab). 💉
- Choriocarcinoma ➝ highly chemo-sensitive (methotrexate, EMA-CO). 🌟
- Testicular cancer ➝ BEP chemo regimen (Bleomycin, Etoposide, Cisplatin). ⚡
- Breast ➝ systemic chemo, hormonal therapy, targeted (HER2 agents). 🎀
- Surgical resection (metastasectomy): Occasionally considered in limited disease ➝ e.g., osteosarcoma. 🔪
- Palliative care: Dyspnoea control (oxygen, opioids), pain management. 🕊️
📉 Prognosis
Generally poor ➝ indicates advanced systemic disease.
⏳ Prognosis varies by tumour biology:
🌟 Testicular cancer ➝ curable, even with cannonball mets (5-year survival >80%).
⚠️ RCC, sarcoma, breast, colon ➝ worse outcomes, dependent on systemic control.
💔 Prognosis linked more to primary cancer type & treatment response than lung disease itself.
