Related Subjects:
|Testicular Torsion
|Paraphimosis
|Hypospadias
|Phimosis
|Balanitis (Children)
🚨 Testicular Torsion: A surgical emergency. The "Golden Hour" for salvage is within 4–6 hours of pain onset.
⚖️ The Rule: Any sudden-onset scrotal pain is torsion until proven otherwise by surgical exploration.
🚫 Do NOT delay for Ultrasound if clinical suspicion is high (NICE/GIRFT 2026).
| 🚨 Emergency Management Pathway (GIRFT 2026) |
- Immediate Priority: Fast-track to Urology/Paediatric Surgery. Do not wait for a senior review if the junior is suspicious.
- Clinical Trigger: Sudden onset pain + absent cremasteric reflex + high-riding/horizontal testis.
- Pre-op: Nil by mouth (NBM), IV fluids, and strong analgesia (e.g., IV Morphine). Do not let pain management delay the surgical call.
- The 1-Hour Rule: National target is surgery within 60 minutes of the decision to operate.
|
🩺 The TWIST Score (Clinical Prediction)
Used to stratify risk without imaging (PPV for torsion is 100% with a score of 6-7):
- Testicular Swelling (2 pts)
- Hard Testis (2 pts)
- Absent Cremasteric Reflex (1 pt)
- Nausea/Vomiting (1 pt)
- High-riding Testis (1 pt)
👉 Score ≥5: High risk-proceed directly to theatre. Score 0-2: Low risk-consider differentials.
🔍 Differential Diagnosis (Acute Scrotum)
| Condition |
Distinguishing Features |
| Testicular Torsion |
Sudden pain, absent cremasteric reflex, high-riding testis, nausea. |
| Torsion of Appendix Testis |
Gradual onset, present cremasteric reflex, "blue dot sign" on superior pole. |
| Epididymo-orchitis |
Gradual onset, fever, dysuria, present cremasteric reflex. (Rare in pre-pubertal boys). |
| Fournier's Gangrene |
Medical emergency-spreading erythema, crepitus, systemic sepsis. |
🛠️ Surgical Principles
- Exploration: Midline or hemiscrotal incision to untwist the cord.
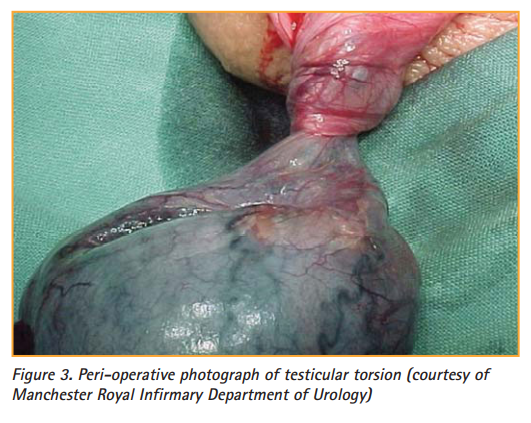
- Viability Check: Warm soaks for 10–20 mins. If pinks up → save; if black/necrotic → Orchidectomy.
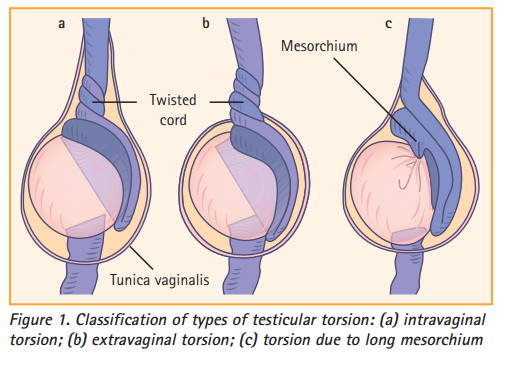
- Fixation (Orchidopexy): Both sides must be fixed (3-point fixation with non-absorbable sutures) because the anatomical "Bell Clapper" deformity is usually bilateral.
⚠️ Critical Tips & Pearls
- The "Intermittent Torsion" Trap: A patient whose severe pain suddenly resolves has likely spontaneously detorted. They are at extreme risk of re-torsion and still require urgent elective orchidopexy. Do not discharge them without surgical review.
- Manual Detorsion: The "Open Book" method (rotating the testis outward like opening a book) can be tried if surgery is delayed, but it is extremely painful and **never** replaces the need for surgery.
- Referred Pain: Always palpate the scrotum in any young male presenting with lower abdominal pain. Torsion often presents as isolated abdominal/groin pain.
- Neonatal Torsion: Usually "extravaginal" and often occurs in utero. If the testis is hard/fixed at birth, salvage is unlikely, but exploration is still usually performed.
📊 Salvage Rates vs. Time
- <6 hours: ~90-100% salvage.
- 6–12 hours: ~50% salvage.
- 12–24 hours: ~20% salvage.
- >24 hours: 0-10% (Orchidectomy likely).
📚 References
