
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
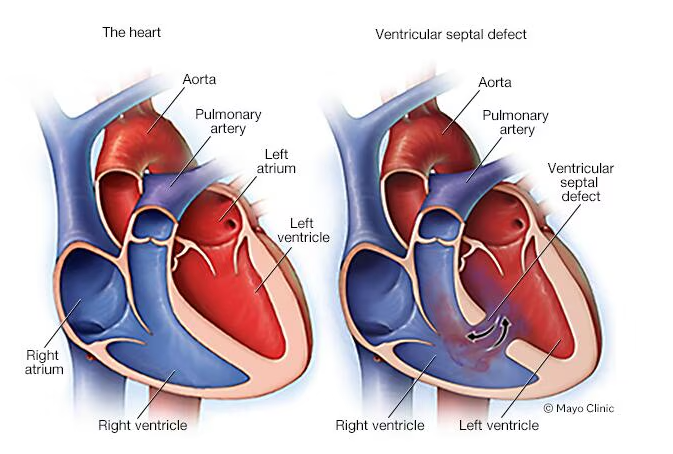
Ventricular Septal defect (VSD) ❤️
Related Subjects: |Congenital Acyanotic Heart Disease |Congenital Cyanotic Heart Disease |Cardiac Embryology |Cyanosis - Central and Peripheral |Down's syndrome (Trisomy 21) |Tetralogy of Fallot |Patent Foramen Ovale (PFO) |Ventricular Septal defect (VSD)
🫀 Ventricular Septal Defect (VSD) is the most common congenital heart defect (≈2/1000 live births). Small VSDs often 🎶 produce loud murmurs but are well tolerated, while large VSDs may be quieter but cause heart failure by 6–8 weeks. Many small muscular defects close spontaneously.
📌 About
- Abnormal shunt between LV → RV.
- Classic finding: harsh pansystolic murmur ± thrill at lower left sternal edge.
- Symptomatic infants: poor weight gain, tachypnoea, feeding fatigue.
🧬 Aetiology & Pathophysiology
- Size of defect + pulmonary pressures dictate severity.
- Large, uncorrected defects → pulmonary hypertension → reversal of shunt = Eisenmenger’s syndrome (cyanosis, clubbing, ↓ murmur).
- High risk of endocarditis – vigilance required.
🔎 Anatomical Types
- Perimembranous – most common; near valves; may close spontaneously; risk aortic regurgitation.
- Muscular – “Swiss cheese”; high chance of closure.
- Inlet (AV canal) – linked with Down syndrome; often surgical.
- Outlet (subarterial) – more frequent in Asia; risk aortic cusp prolapse → early surgery.
- Gerbode – rare LV→RA defect.
🩺 Clinical Features
- 🎶 Loud pansystolic murmur ± thrill (small VSD louder than large).
- Hyperdynamic apex beat, pulmonary overcirculation signs.
- Failure to thrive, recurrent chest infections.
- Eisenmenger’s: RV lift, cyanosis, murmur softens/disappears.
🧪 Investigations
- Bloods: FBC (anaemia), CRP/ESR if ?endocarditis.
- CXR: Normal in small; cardiomegaly & pulmonary plethora in large.
- ECG: Normal if small; LVH + RVH if large.
- Echocardiography: 🥇 gold standard – defect site, shunt size, PA pressure.
💊 Management
- Observation 👀: Most small VSDs close spontaneously → regular follow-up.
- Medical: Diuretics, ACE inhibitors, digoxin for symptomatic infants awaiting repair.
- Surgical Repair 🩻: Patch closure for large, symptomatic, or failing to thrive defects (often in early childhood).
- Device Closure: Via catheter – mainly muscular VSDs.
- Endocarditis Prophylaxis: NICE: only if previous endocarditis or prosthetic material used. But clinicians must remain alert 🚨.
- Long-term follow-up: Monitor for arrhythmias, residual defects, pulmonary hypertension.
⚠️ Complications
- Infective endocarditis
- Heart failure & pulmonary hypertension
- Arrhythmias (esp. post-surgery)
- Eisenmenger’s syndrome
🔍 Comparison: ASD vs VSD vs PDA
| Feature | ASD | VSD | PDA |
|---|---|---|---|
| Definition | Abnormal communication between atria (usually secundum type). | Shunt between LV → RV (most common congenital defect). | Persistent communication between aorta & pulmonary artery. |
| Murmur | 🌬️ Fixed split S2 + ejection systolic murmur (↑ flow across pulmonary valve). | 🎶 Harsh pansystolic murmur ± thrill at LLSB (small = louder). | 🔄 Continuous “machinery” murmur below left clavicle. |
| Clinical Features | Often asymptomatic in childhood; recurrent chest infections; exercise intolerance in adults. | Failure to thrive, HF by 6–8 weeks if large; recurrent chest infections; FTT. | Bounding pulses, wide pulse pressure, HF in infancy if large. |
| ECG | RAD, RBBB pattern (esp. secundum ASD). | LVH ± RVH in large defects; normal if small. | LVH ± RVH in large ducts. |
| CXR | Cardiomegaly, prominent pulmonary arteries. | Small: normal; Large: cardiomegaly, pulmonary plethora. | Cardiomegaly, ↑ pulmonary markings. |
| Complications | Paradoxical emboli, pulmonary hypertension, arrhythmias (AF). | Endocarditis, Eisenmenger’s, arrhythmias, HF. | Endocarditis, Eisenmenger’s (late), HF. |
| Management | Device/surgical closure if large shunt or symptomatic. | Observe if small; surgery/device closure if symptomatic/large. | Indomethacin/ibuprofen (in neonates) or surgical/device closure if persistent. |
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery