
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Tetralogy of Fallot ✅
Related Subjects: |Congenital Acyanotic Heart Disease |Congenital Cyanotic Heart Disease |Cardiac Embryology |Cyanosis - Central and Peripheral |Down's syndrome (Trisomy 21) |Tetralogy of Fallot |Patent Foramen Ovale (PFO) |Ventricular Septal defect (VSD) |Tricuspid Atresia |Transposition of the great arteries (TGA)
💔 Tetralogy of Fallot (TOF) is a common cyanotic congenital heart defect. Some babies are relatively “pink” at birth, while others are cyanosed early depending on how severe the right ventricular outflow tract obstruction (RVOTO) is. Classic features include cyanosis, a harsh ejection systolic murmur, and episodes of sudden worsening cyanosis called hypercyanotic (“Tet”) spells.
📖 About Tetralogy of Fallot
- 🫀 TOF is one of the commonest cyanotic congenital heart defects.
- 🔵 Cyanosis results from reduced pulmonary blood flow and right-to-left shunting across a large ventricular septal defect.
- 👶 Some infants are not markedly cyanosed at birth, but cyanosis may become more obvious over the first weeks or months as dynamic or fixed RVOTO becomes more important.
- 🚨 Hypercyanotic spells are often triggered by crying, feeding, distress, dehydration, fever, or waking.
🧩 The 4 Classic Defects
- 🕳️ Large ventricular septal defect (VSD) – usually non-restrictive.
- 🚧 Right ventricular outflow tract obstruction – often subpulmonary / infundibular, sometimes involving the pulmonary valve.
- 🔄 Overriding aorta – the aorta sits over the VSD and receives blood from both ventricles.
- 💪 Right ventricular hypertrophy (RVH) – develops because the RV pumps against the obstruction.
🔬 Pathophysiology
- ⬇️ RV outflow obstruction reduces blood flow to the lungs.
- ↔️ Because the VSD is usually large, blood can pass from the right ventricle across the VSD into the aorta.
- 🔵 The more severe the RVOTO, the greater the right-to-left shunt and the worse the cyanosis.
- 🫁 Reduced pulmonary blood flow means less oxygenation of blood in the lungs.
- 🖐️ Chronic hypoxaemia can lead to clubbing and poor exercise tolerance.
📊 Diagram
🩺 Clinical Features
- 🔵 Cyanosis – may be mild initially or obvious from early infancy.
- 🍼 Poor feeding, sweating, or tiring easily with feeds.
- 📉 Poor growth / faltering weight gain.
- 🏃 Exercise intolerance in older children.
- 🎧 Harsh ejection systolic murmur at the left upper sternal edge due to RVOT turbulence.
- 🔇 Soft or single second heart sound because pulmonary flow is reduced.
- 🚨 Hypercyanotic (“Tet”) spells – sudden episodes of deepening cyanosis, irritability, tachypnoea, limpness, or collapse.
- 🧎 Older children may squat instinctively after exertion to increase systemic vascular resistance and reduce right-to-left shunting.
- 🖐️ Clubbing may develop in longstanding cyanosis.
🚨 Hypercyanotic (“Tet”) Spells
A Tet spell is a paediatric emergency caused by a sudden increase in right-to-left shunting, usually because pulmonary blood flow falls abruptly. This can happen due to infundibular spasm, reduced preload, or adrenergic stress. The child becomes more cyanosed and distressed, which can worsen the spell further unless it is broken quickly.
| Management of a Tet Spell (Hypercyanotic Spell) |
|---|
|
🧪 Investigations
- 🩻 Echocardiography – the key diagnostic test; defines the anatomy, severity of RVOTO, pulmonary arteries, and associated lesions.
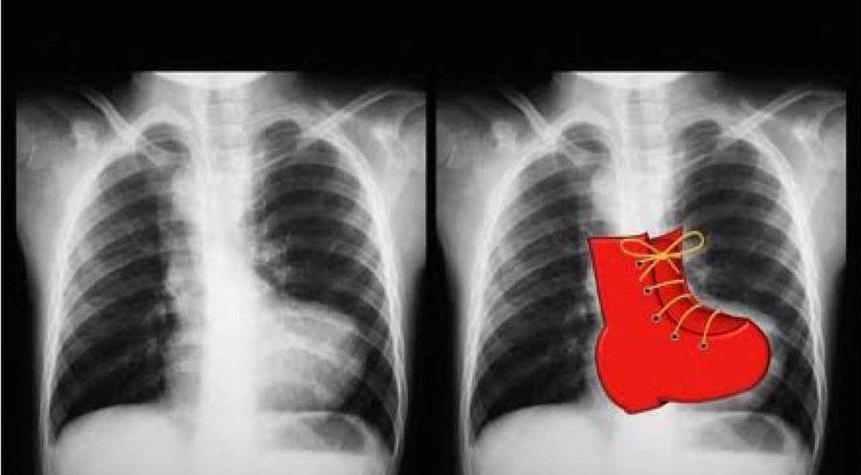
- 📸 Chest X-ray – may show a boot-shaped heart (“coeur en sabot”) and reduced pulmonary vascular markings.
- 📉 ECG – right axis deviation and right ventricular hypertrophy are typical.
- 🧲 Cardiac MRI / CT – useful for detailed anatomical assessment and surgical planning, especially later in follow-up.
- 🩸 Blood tests – may show secondary polycythaemia in longstanding cyanosis.
👶 Newborn and Infant Management
- 🏥 All babies with suspected TOF need early paediatric cardiology assessment.
- 💉 Prostaglandin E1 may be needed in neonates with severe RVOTO or duct-dependent pulmonary blood flow; it is not automatically required in every newborn with TOF.
- 🍼 Optimise feeding, hydration, growth, and oxygenation.
- 🚨 Recurrent hypercyanotic spells are an indication for urgent reassessment and may accelerate timing of intervention.
🔪 Definitive Treatment
- 🥇 Complete surgical repair is the standard treatment.
- 🫀 Repair usually includes VSD closure and relief of RV outflow obstruction.
- 👶 Timing is usually in infancy, depending on symptoms, anatomy, oxygen saturations, and centre practice.
- 🪢 A systemic-to-pulmonary shunt may be used as palliation in selected infants who are too small or unstable for primary repair.
🩹 Long-Term Follow-Up
- 📅 Even after successful repair, patients need lifelong congenital cardiology follow-up.
- 🫀 Important late problems include:
- pulmonary regurgitation
- right ventricular dilatation or dysfunction
- residual RVOTO
- arrhythmias
- exercise limitation
- need for pulmonary valve replacement or further intervention
- ⚡ Adults with repaired TOF remain at risk of atrial and ventricular arrhythmias.
🦷 Infective Endocarditis Advice
- 🪥 Emphasise excellent oral hygiene and regular dental care.
- 📘 NICE does not recommend routine antibiotic prophylaxis for dental procedures.
- 🩺 If there is uncertainty in a high-risk congenital heart patient, seek specialist cardiology / dental advice rather than assuming antibiotics are always required.
⚠️ Exam Red Flag: A child who becomes suddenly more cyanosed and then squats or improves with knee–chest positioning has classic physiology of a Tet spell. 📸 A boot-shaped heart on chest X-ray is another classic clue.
🧠 High-Yield Teaching Points
- 🎓 TOF cyanosis is mainly driven by the severity of RV outflow obstruction.
- 🎓 The VSD is usually large and non-restrictive, so shunting depends on pressure relationships rather than VSD size.
- 🎓 Squatting or knee–chest positioning helps by increasing systemic vascular resistance, reducing the right-to-left shunt.
- 🎓 Repaired TOF is not “cured forever” - lifelong follow-up matters because of pulmonary regurgitation, RV failure, and arrhythmias.
🩺 Case 1 – Infant with Cyanotic Spells
A 6-month-old boy is brought to the emergency department with episodes of sudden cyanosis and breathlessness when crying, relieved by knee–chest positioning. On examination he has a harsh ejection systolic murmur at the left upper sternal edge and central cyanosis. Management: 🚑 Treat as a hypercyanotic spell: calm the child, knee–chest position, oxygen, urgent paediatric review, fluid support if needed, and hospital-based medication according to paediatric cardiology guidance. Definitive treatment is surgical repair. Avoid: ❌ Avoid dehydration and delays in specialist assessment in a symptomatic infant.
🩺 Case 2 – Child with Growth Delay
A 5-year-old girl presents with poor growth, exercise intolerance, cyanosis on exertion, and clubbing. Echocardiography confirms TOF with significant RVOT obstruction. Management: 🩺 Cardiology review, nutritional support, monitor oxygen saturations and haematocrit, and plan definitive repair if not yet repaired. Avoid: ❌ Do not imply routine antibiotic prophylaxis for dental procedures; follow NICE guidance and emphasise oral health.
🩺 Case 3 – Adult with Repaired TOF
A 28-year-old man who had childhood TOF repair presents with palpitations and reduced exercise tolerance. ECG shows right bundle branch block, and imaging shows pulmonary regurgitation with right ventricular dilatation. Management: 💊 Lifelong adult congenital heart disease follow-up, rhythm surveillance, and assessment for pulmonary valve replacement if indicated. Avoid: ❌ Loss to specialist follow-up - repaired TOF patients remain at risk of arrhythmias, RV dysfunction, and re-intervention.
📚 References
- NICE Clinical Guideline CG64: Prophylaxis against infective endocarditis.
- NHS Greater Glasgow and Clyde Paediatric Guideline: Hypercyanotic episodes in tetralogy of Fallot.
- Leeds Teaching Hospitals NHS Trust: Tetralogy of Fallot in children.
- ESC Guidelines: Adult Congenital Heart Disease.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery