
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Helicobacter pylori
📚 Related Subjects: | Listeriosis | Moraxella catarrhalis | Leptospira interrogans | Lactobacillus acidophilus | Helicobacter pylori | Haemophilus parainfluenzae | Haemophilus influenzae
🎯 Treatment of H. pylori aims to eradicate infection, reduce peptic ulcer disease and bleeding risk, and prevent recurrence, gastric cancer, and MALT lymphoma.
📖 About
- Discovered by Barry Marshall & Robin Warren in 1982 🧪.
- Most common cause of peptic ulceration, though many carriers are asymptomatic.
- Present in ~95% of duodenal ulcers and 70–80% of gastric ulcers.
- NSAIDs + H. pylori = 🔥 high ulcer risk.
- Associated with acute/chronic gastritis, gastric adenocarcinoma, and MALT lymphoma (regresses after eradication in many cases).
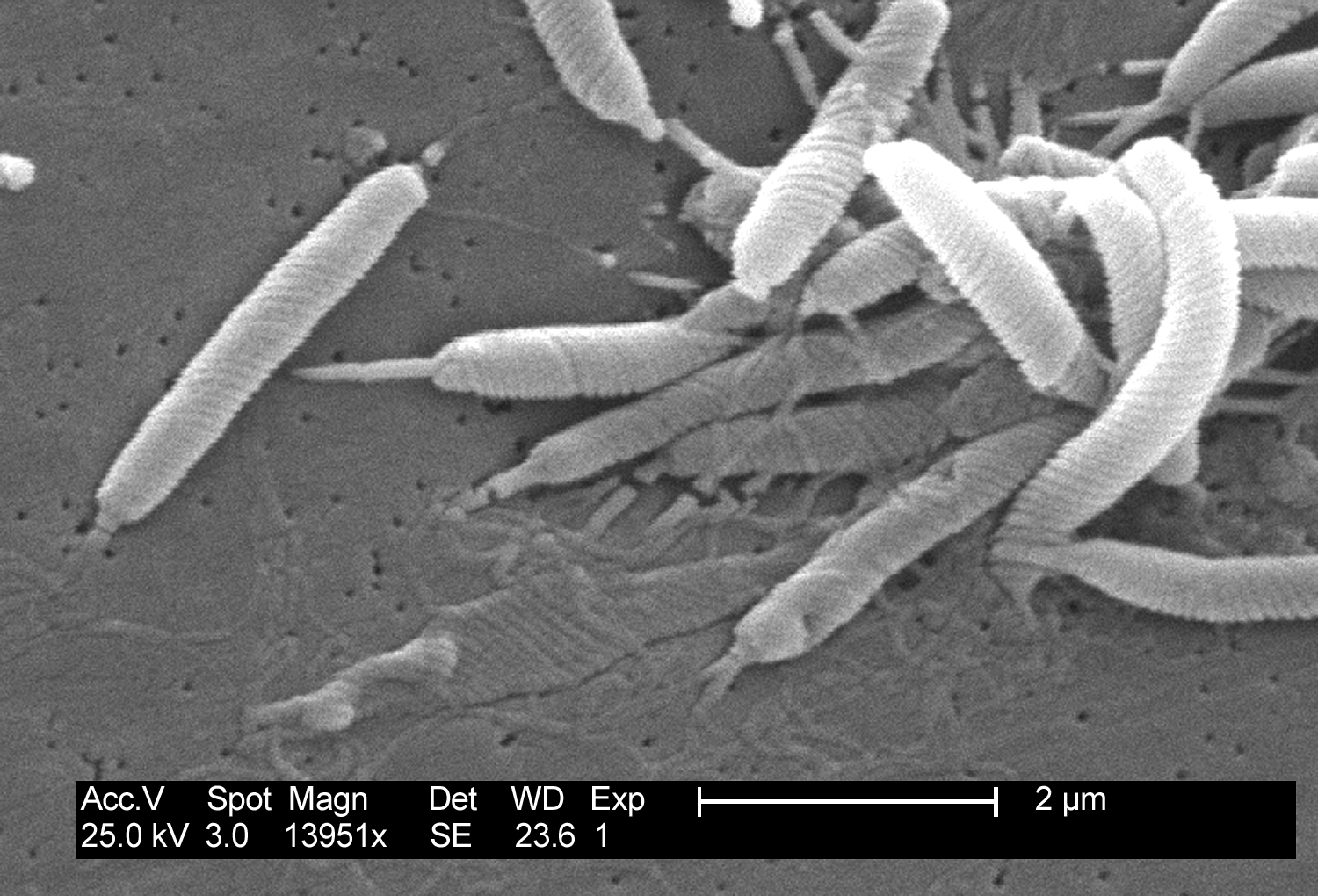
🔬 Electron Microscopy
🌍 Source
- Spread mainly person-to-person → oral–oral or faeco–oral.
- More common in older adults and in lower socioeconomic groups.
- Humans are the main reservoir (occasionally found in cats 🐈).
⚙️ Characteristics
- Spiral-shaped, Gram-negative, highly motile bacillus.
- Microaerophilic with 4–6 unipolar flagella.
- Urease production → breaks down urea to ammonia → neutralises gastric acid locally.
- Lives beneath gastric mucous layer and adheres to epithelial cells.
🧨 Virulence
- Causes neutrophilic gastritis.
- CagA gene linked to severe disease and higher gastric cancer risk.
- Produces urease and VacA toxin → epithelial injury.
🩺 Pathogenicity
- Antral gastritis → achlorhydria + ↑ gastrin + ↑ acid secretion.
- Chronic duodenal ulcers (95% cases) & gastric ulcers (70–80%).
- Gastric cancer: adenocarcinoma (80% linked to H. pylori).
- MALT lymphoma: may regress after eradication.
🧪 Investigations
- 🩸 Serology: Detects IgG → cannot distinguish past from current infection.
- 💨 Urea Breath Test (13C/14C): Most accurate non-invasive test.
- 💩 Stool Antigen Test (SAT): Confirms active infection.
- 🔬 Histology + biopsy urease (CLO test): High sensitivity/specificity.
- 🧫 Culture: Gold standard but slow (used for resistance testing).
🧾 NICE/CKS testing rule (important): for UBT or stool antigen, stop PPI for 2 weeks and avoid antibiotics for 4 weeks beforehand (false negatives otherwise). If you must treat symptoms, consider an H2 blocker/antacid short-term and re-test later.
💊 Management (UK – NICE/BNF-aligned)
- First-line (Triple Therapy): for 7 days (choose based on prior antibiotic exposure)
- PPI BD (e.g., omeprazole 20 mg BD or equivalent)
- Amoxicillin 1 g BD
- Either clarithromycin 500 mg BD OR metronidazole 400 mg BD
- Penicillin allergy (Triple Therapy): for 7 days
- PPI BD (e.g., omeprazole 20 mg BD or equivalent)
- Clarithromycin 250 mg BD
- Metronidazole 400 mg BD
- Second-line (if failure / persistent symptoms): for 7 days (switch the antibiotic not used first-line)
- PPI BD (e.g., omeprazole 20 mg BD or equivalent)
- Amoxicillin 1 g BD
- Either clarithromycin 500 mg BD OR metronidazole 400 mg BD - choose the one not used first line
- When eradication is indicated:
- Peptic ulcer disease (gastric & duodenal)
- MALT lymphoma
- Post-bleed ulcers & atrophic gastritis
- Routine screening for asymptomatic carriers is not recommended in low-risk groups.
✅ Confirm eradication (test-of-cure) & follow-up (NICE/CKS aligned)
🔁 Don’t “assume cured”. If re-testing is indicated, use a 13C urea breath test or stool antigen test (not serology), and time it correctly to avoid false negatives. NICE quality standards emphasise a 2-week PPI washout before testing, and CKS advises waiting long enough after antibiotics.
- Who should have a test-of-cure? (common UK indications)
- 🩸 Peptic ulcer disease (gastric or duodenal), especially if complicated (bleed/perforation) or high-risk recurrence.
- 🎗️ MALT lymphoma (proof of eradication is essential as it can drive remission).
- 🧪 Persistent or recurrent symptoms after eradication therapy (particularly if initial testing conditions were suboptimal).
- 💊 High concern about failure (poor adherence, prior macrolide/metronidazole exposure, suspected resistance).
- When to re-test (timing rules):
- ⏱️ Arrange re-testing at least 4 weeks after completing eradication antibiotics (ideally 8 weeks in many pathways).
- ⛔ Stop PPI for 2 weeks before the breath test / stool antigen test (NICE QS96).
- ⛔ Avoid antibiotics for 4 weeks before testing (CKS advice) to reduce false negatives.
- Choice of test:
- 💨 13C urea breath test = excellent non-invasive “test-of-cure”.
- 💩 Stool antigen test = also confirms active infection and is suitable for “test-of-cure”.
- 🩸 Serology is not appropriate for confirmation (IgG can stay positive for months/years).
- What if symptoms persist but test-of-cure is negative?
- Consider functional dyspepsia, GORD, ongoing NSAID injury, biliary disease, pancreatitis, malignancy, or alternative infection.
- If alarm features develop (weight loss, dysphagia, GI bleed, anaemia, persistent vomiting): follow urgent endoscopy pathways.
- What if the test-of-cure is positive (treatment failure)?
- ✅ Check adherence, dosing, and whether the patient was on a PPI at the time of testing.
- 🔁 Use a different second-line regimen (usually switching the antibiotic not used first-line) per CKS/local antimicrobial guidance.
- 🧫 After ≥2 failures, consider endoscopy for culture/susceptibility and specialist input (local pathway).
- Gastric ulcer follow-up (important NICE/CKS point):
- 🩻 Ensure all patients with a proven gastric ulcer have repeat endoscopy to confirm healing and exclude malignancy; arrange H. pylori re-testing if appropriate (CKS).
📚 Guideline links (UK)
- NICE QS96: 2-week PPI washout before H. pylori testing
- NICE CKS: Dyspepsia (unidentified cause) – H. pylori test/treat + re-test timing
- NICE CKS: Proven peptic ulcer – repeat endoscopy for gastric ulcer + H. pylori follow-up
- UK “Test and treat” quick reference (PHE/NICE-linked PDF)
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery