
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Coeliac disease ✅
Related Subjects: |Colorectal cancer |Colorectal polyps |Ulcerative Colitis |Acute Severe Colitis |Crohn's disease |Coeliac disease |Familial Adenomatous polyposis (FAP) |Surgical Stomas
⚠️ Coeliac disease carries an increased risk of malignancy (especially enteropathy-associated T-cell lymphoma, small bowel adenocarcinoma, and squamous cell carcinoma of the oropharynx/oesophagus). 👉 New or unexplained symptoms in a diagnosed patient should always prompt review, as they may indicate complications or malignant transformation.
ℹ️ About
- Coeliac disease is a chronic autoimmune enteropathy triggered by dietary gluten (found in wheat, rye, barley).
- Prevalence ≈ 1 in 100 in Western populations; in the UK, incidence ≈ 1 in 2000, highest in western Ireland (≈ 1 in 300).
- Can present at any age – adults with new GI or systemic symptoms should be considered for testing.
🧬 Aetiology & Pathophysiology
- Immune reaction to α-gliadin → T-cell mediated release of interferon-γ → villous atrophy, crypt hyperplasia, and lymphocytic infiltration.
- Strong genetic predisposition: 95% carry HLA-DQ2 or HLA-DQ8.
- Associated autoimmune conditions: type 1 diabetes, autoimmune thyroid disease, autoimmune liver disease.
🧒 Clinical Features
- Infants/young children: Failure to thrive, abdominal distension, abnormal stools, anaemia, irritability.
- Older children/adults: Fatigue, diarrhoea, steatorrhoea, abdominal pain, weight loss, headaches, arthralgia.
- Extra-intestinal features: Iron/folate deficiency anaemia, osteoporosis/osteomalacia, infertility, neurological manifestations (peripheral neuropathy, ataxia).
- Dermatitis herpetiformis: Intensely itchy rash on elbows, knees, and buttocks; pathognomonic for coeliac disease.
🧪 Investigations
- Blood tests: FBC, iron/folate/vitamin B12, calcium, phosphate, ALP, albumin, PT/INR. Howell–Jolly bodies may indicate hyposplenism.
- Serology: IgA anti-tTG (first-line, high sensitivity/specificity), total IgA to rule out IgA deficiency, anti-endomysial antibodies if needed.
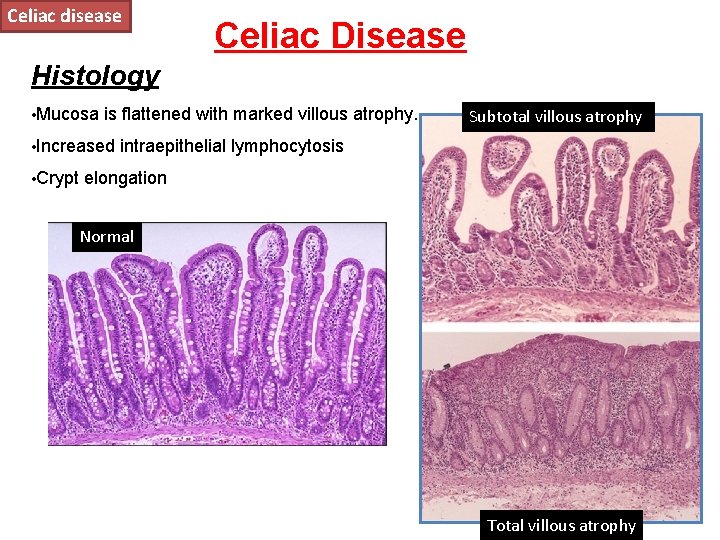
- Endoscopy + biopsy: Multiple duodenal biopsies show villous atrophy, crypt hyperplasia, and intraepithelial lymphocytosis (gold standard).
🔍 Differentials
- Tropical sprue, cystic fibrosis, milk protein enteropathy.
- Infective: Giardiasis.
- Other: chronic pancreatitis, abetalipoproteinaemia.
💊 Management
- Gluten-free diet (GFD): Lifelong adherence is cornerstone. Monitor antibody titres for adherence.
- Nutritional supplementation: Iron, folate, calcium, vitamin D, and fat-soluble vitamins as required.
- Refractory cases: Short course of corticosteroids or immunosuppressants if strict GFD fails.
- Family screening: First-degree relatives should be considered for testing.
- Follow-up: Monitor growth in children, bone health, antibody titres, and symptoms; re-biopsy only if symptoms persist.
⚠️ Complications
- Growth retardation and delayed puberty in children.
- Osteopenia, osteoporosis, and osteomalacia due to malabsorption.
- Malignancy: enteropathy-associated T-cell lymphoma, small bowel adenocarcinoma, oesophageal SCC.
- Hyposplenism → risk of overwhelming sepsis (vaccinate against encapsulated organisms).
📌 Key Teaching Points
- Always test for coeliac disease before diagnosing IBS in adults.
- Do not start a gluten-free diet before biopsy confirmation – can normalize histology and obscure diagnosis.
- Vaccinate against pneumococcus if hyposplenic.
- Long-term follow-up essential: monitor nutrition, bone density, and malignancy risk.
Cases – Coeliac Disease
- Case 1 (Classic pediatric): 9-year-old boy with chronic diarrhoea, abdominal distension, faltering growth, iron-deficiency anaemia, low vitamin D. Anti-tTG IgA raised; duodenal biopsy confirms villous atrophy. Management: Lifelong GFD, dietitian support, iron & vitamin D supplementation. Outcome: Growth improves, anaemia resolves, antibody titres fall.
- Case 2 (Atypical adult): 42-year-old woman with fatigue, aphthous ulcers, refractory iron-deficiency anaemia, no GI symptoms. Anti-tTG positive; biopsy confirms coeliac disease. Management: Gluten-free diet, nutrition counselling, iron replacement. Outcome: Symptom improvement and normal Hb after 4 months.
- Case 3 (Silent/subclinical): 55-year-old man with osteoporosis after low-impact fracture, mild anaemia, elevated anti-tTG, villous blunting on biopsy. Management: Gluten-free diet, calcium & vitamin D, bisphosphonate therapy. Outcome: Bone density stabilises, anaemia improves, patient educated on strict diet adherence.
Teaching Commentary 🧑⚕️
These cases illustrate the spectrum of coeliac disease:
1) Classic malabsorptive form in children.
2) Atypical/extra-intestinal presentation in adults.
3) Silent/subclinical disease detected through complications like osteoporosis.
The disease is immune-mediated, triggered by gluten peptides, leading to villous atrophy. Management is always a lifelong gluten-free diet with dietitian support. Monitor for deficiencies, bone health, and malignancy risk. Early recognition prevents irreversible complications.
📚 References
- NICE Guideline: Coeliac Disease – Recognition, Assessment and Management (NG20)
- Coeliac UK – Information & Resources
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery