Related Subjects:
|Transient Loss of Consciousness
|Vasovagal Syncope
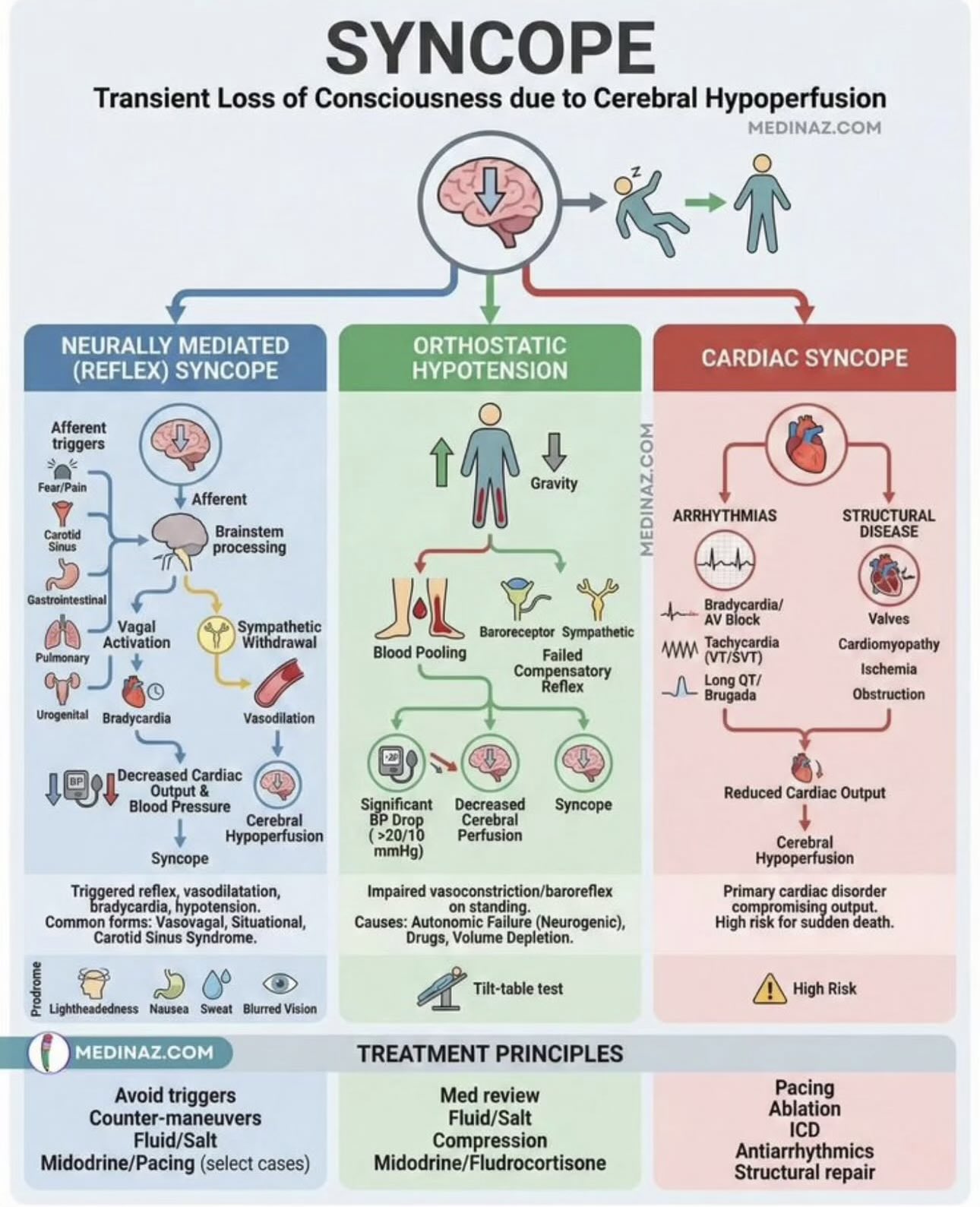
|Syncope
|Aortic Stenosis
|First Seizure
|Carotid Sinus Syncope
⚡ Immediate management: Lay the patient flat and raise their legs to increase cerebral blood flow.
ℹ️ About
- 🧠 Syncope = transient loss of consciousness (TLOC) due to inadequate cerebral perfusion.
⚙️ Pathophysiology
- BP = CO × PR.
- ⬇️ Peripheral resistance (PR): vasodilation, anaphylaxis, vasodilators (e.g. GTN).
- ⬇️ Cardiac output (CO = HR × SV): arrhythmias, aortic stenosis, hypovolaemia.
🧾 Clinical Features
- ⚠️ Warning symptoms? e.g. tinnitus, visual dimming, impending blackout.
- 🩺 Pain or breathlessness before event?
- 💥 Collapse ➝ how quickly did recovery occur? Injury? Incontinence?
🗂️ Causes of Syncope
| Type | Details |
|---|
| 🙈 Vasovagal |
Situational (church, standing, hot bath, toilet, venesection).
Prodrome: tinnitus, dimmed vision, pallor, impending faint.
Recovery: rapid once supine, patient flushed & sweaty but not confused. May jerk or pass urine. |
| 📉 Postural |
Fainting on standing ➝ autonomic dysfunction, hypovolaemia, salt depletion, or antihypertensives/antianginals. |
| ❤️ Arrhythmias |
Bradycardia or tachycardia reduce CO.
Loss of consciousness irrespective of posture.
Stokes-Adams attack = sudden loss of ventricular contraction (progression to complete heart block). |
| 👔 Carotid sinus syncope |
Elderly; hypersensitive carotid sinus.
Trigger: tight collar/light pressure ➝ reflex bradycardia & syncope. |
| 🏃 Exertional syncope |
Aortic stenosis or HCM.
Heart cannot increase CO during exertion. |
❤️ Cardiac Causes (High Risk)
- Severe aortic stenosis.
- Complete heart block or sinus pauses.
- Ventricular tachycardia.
- Stokes-Adams attack.
- Medication-exacerbated vasovagal syncope.
🔍 Clinical Assessment
- ⏱️ History of event: was it truly syncope? Did they appear "dead"?
- ⚡ Recovery speed, any trauma, incontinence, protective reflexes (e.g. outstretched hand).
- 👀 Witness history is essential (phone them if needed).
- 🩸 Check lying/standing BP.
- 🏾 Look for Addison’s disease (hypotension, pigmentation).
- 🎧 Auscultate murmurs (aortic stenosis, HCM).
🧪 Investigations
- Bloods: FBC, U&E, CRP, LFT, calcium, ALP.
- 📉 ECG: arrhythmias, pauses, heart block, tachycardia.
- 🫁 CXR: cardiomegaly, pulmonary disease.
- 🫀 Echo: exclude valve stenosis, cardiomyopathy, poor LV function.
- 🧠 Carotid Dopplers only if focal neurology.
- 📊 Ambulatory ECG (24h–7 day tape, implantable loop recorder).
- 📐 Tilt table test: 60° for 45 min with ECG + BP monitoring.
- 🏃 Exercise stress test (if exertional).
- 🩺 Coronary angiogram if IHD suspected.
💊 Management
- 🔧 Address underlying cause.
- Bradycardia ➝ stop causative drugs, consider pacemaker.
- Exertional syncope with aortic stenosis ➝ surgery/valve replacement.
- Vasovagal ➝ patient education, hydration, avoid triggers.
- Postural ➝ review meds, increase fluids/salt, compression stockings.