Snake Bites
⚠️ Most snake bites in the UK are not serious, but ALL snake bites must be checked by a doctor.
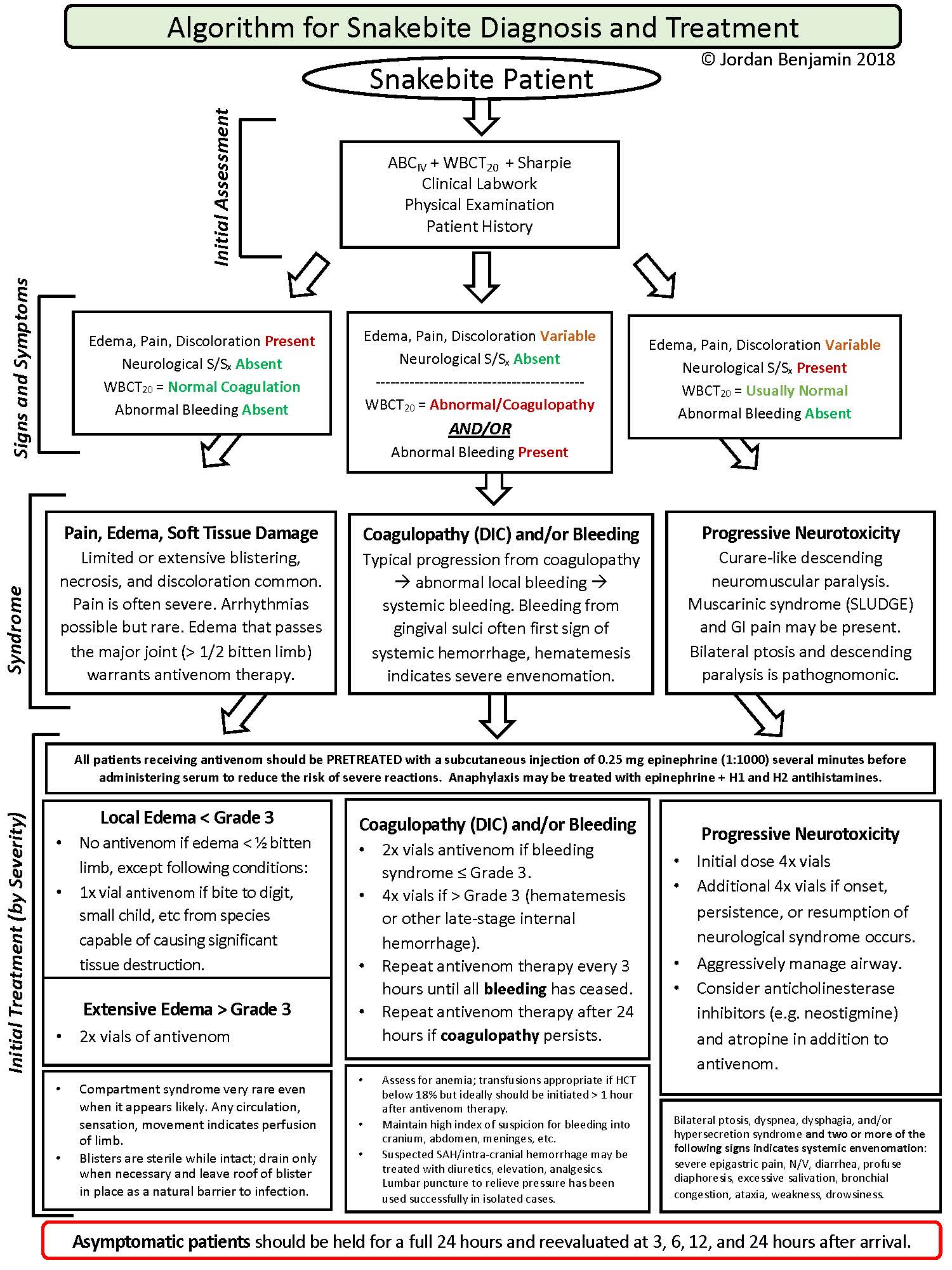
👉 Useful guideline link: Snakebite Treatment Resources
Snakebite: what to do (quick practical)
- 1️⃣ Freeze 🧊 : Keep the person still and calm. Movement increases lymphatic flow and can spread venom faster.
- 2️⃣ Splint 🦴 Immobilise the bitten limb like a fracture (splint + sling if arm). Keep it at heart level (not raised high).
- 3️⃣ Remove jewellery 💍 Rings and watches can become “strangle-wires” as swelling develops.
Watch for red flags
- 🚨 Neurotoxic : Drooping eyelids, slurred speech, weakness → paralysis risk.
- 🚨 Haemotoxic: Bleeding gums, easy bruising, rapidly progressive swelling.
- 🚨 Myotoxic: Severe muscle pain and dark/cola urine (rhabdomyolysis risk).
Key actions + behaviour
- ✅ DO
- Call emergency help immediately (999/112).
-
Keep them still and reassure (panic = movement).
-
Immobilise the limb with a splint; keep it at heart level.
-
Remove rings/watches/tight clothing early.
-
Note the time of the bite and track symptoms (swelling, speech, breathing).
- ⛔ DON’T
- Don’t cut, suck, or wash the wound (worsens injury / removes venom traces).
- Don’t apply a tourniquet (ischaemia + sudden venom bolus when released).
- Don’t use ice or electric shocks (no benefit; tissue harm).
- Don’t let them walk or run “to get help” (carry/assist instead).
- Don’t try to catch the snake (second bite risk).
Why this works (clinical logic)
Many venoms spread mainly via lymphatics, so stillness + immobilisation slows systemic absorption.
Early jewellery removal prevents constriction as oedema develops, and symptom-pattern recognition (neuro/haemo/myo) helps anticipate
airway risk, coagulopathy, or rhabdomyolysis.
.
🌍 About
- Worldwide, ~5.4 million people are bitten by snakes each year, with up to 2.7 million envenomings.
- Most bites occur in Africa, Asia, and Latin America, where snakes and humans are in closer contact.
🐍 Snake Bites in the UK
- The European Adder is the only venomous snake in the UK.
- Adders are grey or reddish-brown with a distinctive dark zig-zag stripe along the back.
- Although bites are rarely fatal, always seek hospital care.
🌎 Dangerous Snakes Worldwide
Some of the world’s most dangerous snakes include:
| 🐍 Snake |
Where Found |
⚡ Danger |
Notes |
| King Cobra |
Southeast Asia, India |
Neurotoxic – respiratory failure |
Largest venomous snake, intimidating hood. |
| Inland Taipan |
Australia |
Most toxic venom worldwide |
"Fierce snake" – rarely bites humans. |
| Russell’s Viper |
South Asia |
Haemotoxic – bleeding, renal failure |
Responsible for many deaths in Asia. |
| Black Mamba |
Sub-Saharan Africa |
Rapidly fatal neurotoxin |
Fast, aggressive, highly feared. |
| Fer-de-Lance |
Central & South America |
Haemotoxic – severe necrosis |
Commonest fatal snake in Central America. |
🧪 Clinical Effects by Venom Type
| Venom Type |
Features |
Management |
| 🩸 Haemotoxic (Vipers) |
Pain, swelling, bruising, bleeding, shock |
Immobilize limb, antivenom, fluids, blood products |
| 🧠 Neurotoxic (Cobras, Kraits, Mambas) |
Ptosis, paralysis, respiratory failure |
Antivenom + respiratory support (ventilation if needed) |
| 💪 Myotoxic (Sea Snakes) |
Muscle pain, dark urine, renal failure |
Antivenom + aggressive IV fluids, monitor electrolytes |
| ❤️ Cardiotoxic (Mambas, Elapids) |
Arrhythmias, cardiac arrest |
Antivenom, cardiac monitoring, ACLS if arrest |
| 🦵 Local Tissue Damage |
Swelling, necrosis, blistering |
Wound care, tetanus, antibiotics, debridement if needed |
⚠️ Complications
- 🧠 Paralysis
- 🩸 Disseminated intravascular coagulation (DIC)
- 🚰 Acute kidney injury (AKI)
- ✂️ Amputation due to necrosis
- 💀 Multiorgan failure
🚑 First Aid & Emergency Management
- ✅ Ensure safety – move away from snake.
- ✅ Keep patient calm & limb immobilized (at or below heart level).
- ✅ Call for emergency help – transfer to hospital quickly.
- ✅ Apply a pressure immobilization bandage (for neurotoxic bites e.g., cobra, mamba).
- ❌ Do NOT use a tourniquet, cut, suck, or apply ice.
- ✅ Monitor vitals (breathing, BP, HR).
- 💉 Give antivenom at hospital – definitive treatment.
- 🧴 Supportive care: IV fluids, analgesia, treat shock, seizures, or respiratory failure.
- 💉 Give tetanus prophylaxis if not up-to-date.
🏥 In-Hospital Care
- Most patients admitted for at least 24h monitoring.
- Wound cleaned, bandaged, supportive care provided.
- Antivenom used if confirmed or suspected envenomation.
📚 References
Cases - Snake Bites 🐍
- Case 1 - Neurotoxic Snakebite (Cobra) 🧠:
A 25-year-old farmer in India presents 2 hours after a bite to the leg. He has drooping eyelids, slurred speech, and difficulty swallowing. Exam: bilateral ptosis, shallow respirations, O₂ sats 84% RA.
Diagnosis: Neurotoxic envenomation (cobra).
Management: Airway support, early antivenom, ICU monitoring, ventilatory support if needed.
- Case 2 - Haemotoxic Snakebite (Viper) 🩸:
A 40-year-old man develops swelling, bleeding gums, and haematuria after a viper bite. Exam: hypotension, oozing from venepuncture sites. Coagulation screen: prolonged PT, low fibrinogen, thrombocytopenia.
Diagnosis: Haemotoxic envenomation causing DIC.
Management: Antivenom, blood products (FFP, cryoprecipitate), IV fluids, renal monitoring.
- Case 3 - Cytotoxic Snakebite (Puff Adder) 🦵:
A 33-year-old safari worker is bitten on the ankle by a puff adder. Rapidly progressive swelling, blistering, and necrosis develop around the wound. Exam: severe pain, compartment syndrome signs.
Diagnosis: Cytotoxic envenomation.
Management: Antivenom, analgesia, wound care, fasciotomy if compartment syndrome, possible grafting later.
- Case 4 - Allergic Reaction to Snakebite 🫁:
A 29-year-old man is bitten by a non-venomous snake but develops sudden urticaria, wheeze, and hypotension minutes later.
Diagnosis: Anaphylaxis to snake venom proteins.
Management: IM adrenaline, IV fluids, antihistamines, steroids, airway support.
- Case 5 - “Dry Bite” (No Envenomation) ✅:
A 21-year-old tourist in Africa is bitten by a snake on the calf. Minimal local pain and swelling; no systemic features after 12 hours observation. Coagulation normal.
Diagnosis: Dry bite (no venom injected).
Management: Wound cleaning, tetanus prophylaxis, observation; reassurance and discharge if stable.
Teaching Commentary 🧠
Snakebites cause different clinical syndromes depending on venom:
- Neurotoxic → paralysis (cobra, krait).
- Haemotoxic → bleeding/DIC (vipers).
- Cytotoxic → local necrosis, compartment syndrome (puff adder).
- Allergic → anaphylaxis.
- Dry bite → no venom, just local effects.
Management priorities:
1️⃣ First aid: immobilise limb, no tourniquets/cutting.
2️⃣ Hospital: airway, breathing, circulation.
3️⃣ Give antivenom if systemic features or severe local swelling.
4️⃣ Supportive: fluids, blood products, analgesia, wound care.
⚠️ Always monitor for late complications: renal failure (haemotoxic), neuropathy (neurotoxic), tissue loss (cytotoxic).
