0️⃣ Definitions - set expectations early
- NSTEMI: symptoms/signs of myocardial ischaemia + rise/fall in troponin indicating myocardial necrosis, without persistent ST elevation.
- Unstable angina: ischaemic symptoms, often with ECG changes, but troponin is not elevated.
- Core goal: stabilise myocardium, prevent thrombus extension, reduce recurrent MI/death, and use risk-based angiography.
1️⃣ Recognition & Immediate Actions - first 10 minutes
- 🎯 Suspect NSTE-ACS with chest pain/pressure, or atypical symptoms such as dyspnoea, collapse, nausea, syncope or epigastric discomfort, especially in older adults, women, diabetes and CKD.
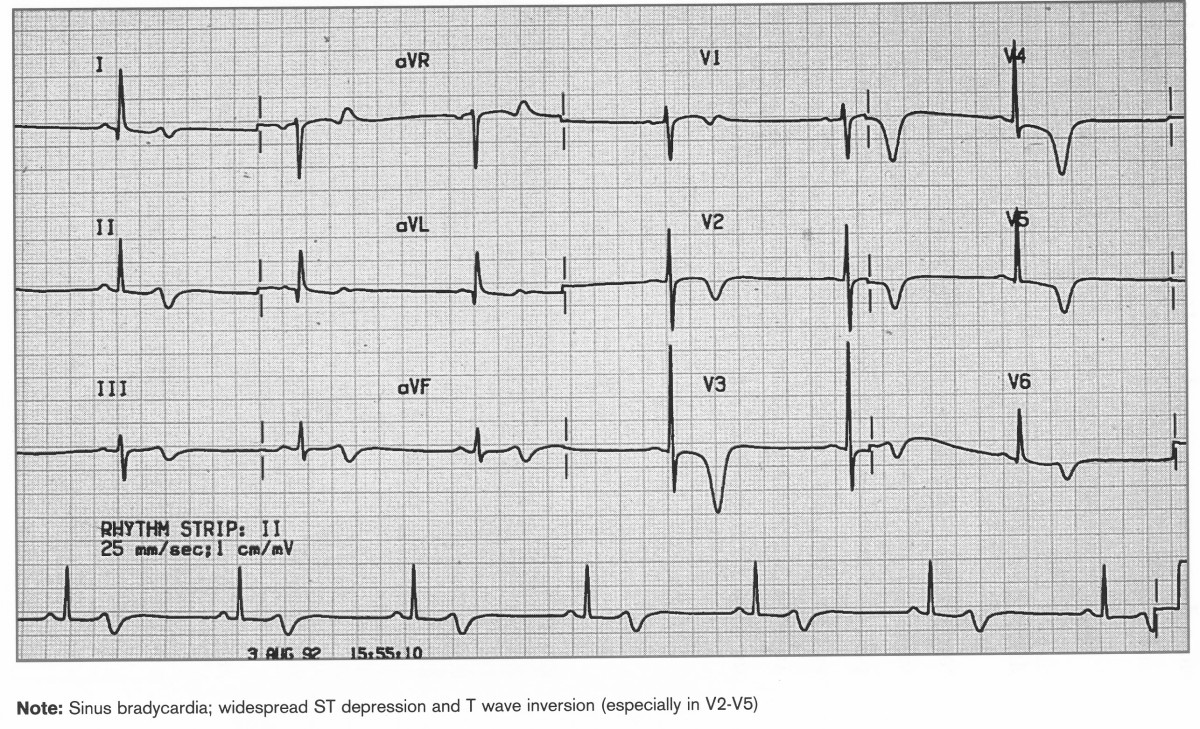
- 📊 Perform a 12-lead ECG immediately; repeat if pain continues, symptoms recur, or the ECG evolves.
- 📟 Use continuous cardiac monitoring/telemetry if ongoing pain, arrhythmia risk, haemodynamic instability or confirmed ACS; ensure defibrillator access ⚡.
- 🫁 Oxygen: give only if hypoxaemic, using local oxygen guidance; usual target 94–98%, or 88–92% if at risk of hypercapnic respiratory failure.
- 💉 Gain IV access, record baseline observations, calculate NEWS2, and check point-of-care glucose.
- 🚫 Do not give dual antiplatelet therapy before the diagnosis of unstable angina or NSTEMI is made; this reduces avoidable bleeding harm in mimics such as aortic dissection, PE or pericarditis.
2️⃣ Investigations - do not delay urgent treatment
- 🧪 Bloods: high-sensitivity troponin, FBC, U&E/creatinine, glucose, clotting, LFTs if clinically useful, and lipids for baseline cardiovascular risk.
- ⏱️ Serial troponin: use the local high-sensitivity troponin pathway, commonly 0/1-hour or 0/2-hour. A dynamic rise and/or fall supports acute myocardial injury/infarction.
- 📷 CXR: consider if an alternative diagnosis or complication is suspected, such as pulmonary oedema, pneumothorax, pneumonia or widened mediastinum; do not allow routine imaging to delay ACS treatment.
- 🫀 LV function: assess in all NSTEMI patients; consider in unstable angina. Echocardiography is also useful if heart failure, murmur, shock, regional wall motion abnormality or mechanical complication is suspected.
- 🔎 Consider mimics selectively: aortic dissection, pulmonary embolism, myocarditis/pericarditis, pneumothorax, oesophageal disease and sepsis-related myocardial injury.
3️⃣ Risk Stratification - NICE uses predicted 6-month mortality
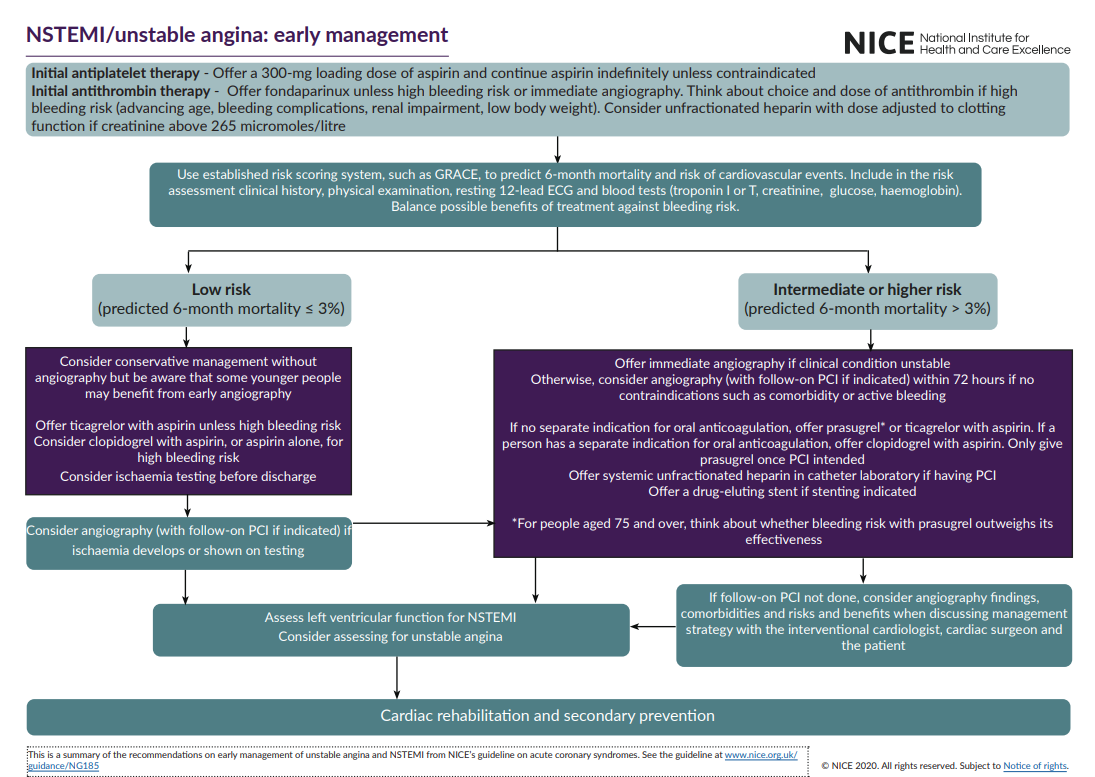
- 📊 Once NSTEMI/unstable angina is diagnosed and aspirin plus antithrombin treatment has been offered, assess risk using a score that predicts 6-month mortality, for example GRACE.
- 🟢 Lowest/low risk: predicted 6-month mortality ≤3% → conservative management may be appropriate if clinically stable.
- 🟠 Intermediate or higher risk: predicted 6-month mortality >3% → consider coronary angiography within 72 hours of first admission if no contraindications.
- 🚨 Unstable or very high-risk features: haemodynamic instability, cardiogenic shock, refractory/recurrent ischaemia, malignant arrhythmia such as VT/VF, acute heart failure or pulmonary oedema → immediate angiography.
4️⃣ Immediate Medical Therapy - anti-ischaemic + antithrombotic
- 💊 Aspirin: give 300 mg loading dose, then continue indefinitely unless contraindicated.
- 💉 Antithrombin treatment - NICE:
- Fondaparinux is usually offered unless immediate coronary angiography is planned, or the bleeding risk is very high.
- Typical ACS dose is fondaparinux 2.5 mg SC daily, but check renal function and local formulary/BNF guidance before prescribing.
- In significant renal impairment, for example creatinine >265 micromol/L, consider unfractionated heparin instead, dose-adjusted to clotting monitoring.
- ⚠️ In high bleeding risk, individualise the agent and dose, considering age, frailty, renal impairment, previous bleeding, anaemia, low body weight and need for oral anticoagulation.
- 🌬️ Nitrates: use GTN sublingual or IV for ongoing ischaemic pain and hypertension if no contraindications. Avoid in hypotension, severe aortic stenosis, suspected RV infarct, or recent PDE5 inhibitor use.
- 💉 Analgesia: give IV opioid titrated to pain with an antiemetic if required.
- 🫀 Beta-blocker: consider early oral beta-blocker if tachycardic or hypertensive and there is no acute heart failure, shock, bradycardia, heart block or active bronchospasm.
- 🧴 High-intensity statin: start early unless contraindicated, following the local post-ACS lipid pathway.
5️⃣ P2Y12 Inhibitor Strategy - NICE NG185
- ⚠️ Timing: avoid routine P2Y12 pretreatment before the diagnosis is confirmed. Once unstable angina or NSTEMI is diagnosed, choose the second antiplatelet according to angiography/PCI plan, bleeding risk and need for oral anticoagulation.
- If coronary angiography is planned:
- If there is no separate indication for ongoing oral anticoagulation, offer prasugrel or ticagrelor with aspirin.
- Prasugrel: give only once coronary anatomy is defined and PCI is intended. Use caution in older adults, low body weight and previous stroke/TIA risk.
- If the person does have a separate indication for ongoing oral anticoagulation, offer clopidogrel with aspirin.
- If PCI is not indicated or conservative management is chosen:
- Offer ticagrelor + aspirin unless bleeding risk is high.
- If high bleeding risk, consider clopidogrel + aspirin or aspirin alone, using senior/specialist judgement.
6️⃣ Invasive Strategy & Timing - NICE
- 🚑 Immediate coronary angiography if the clinical condition is unstable, including shock, refractory ischaemia, life-threatening arrhythmia or acute heart failure.
- 🕒 Otherwise, consider angiography with follow-on PCI if indicated within 72 hours of first admission if predicted 6-month mortality is >3% and there are no contraindications.
- 🩻 PCI practical point: if PCI is performed, offer systemic unfractionated heparin in the catheter laboratory, whether or not fondaparinux has already been given.
- 🧷 If stenting is indicated, offer a drug-eluting stent.
- 🔁 If the revascularisation strategy is unclear, for example PCI versus CABG, discuss in a heart-team format with interventional cardiology, cardiac surgery and the patient.
7️⃣ Supportive Care & Complication Surveillance
- 🛏️ Nurse in a monitored setting until clinically stable; watch for VT/VF, AF, heart block, recurrent ischaemia and haemodynamic deterioration.
- 🌊 Treat heart failure or pulmonary oedema promptly with diuretics, nitrates if appropriate, oxygen/NIV if hypoxaemic, and urgent cardiology or critical care input if severe.
- 🧪 Glucose: aim to keep blood glucose below 11 mmol/L while avoiding hypoglycaemia. Consider dose-adjusted insulin infusion early if needed.
- 🩸 Reduce bleeding risk: review anticoagulants, NSAIDs and antiplatelets; consider gastroprotection if high GI bleeding risk according to local policy.
- 🧠 Re-check the diagnosis if pain is tearing or radiates to the back, or there is neurological deficit, pulse deficit, severe hypertension, hypotension or mediastinal widening → think aortic dissection and avoid antithrombotics until excluded.
8️⃣ Before Discharge - NICE
- 🫀 Assess LV function in all NSTEMI patients and document this clearly in the discharge summary.
- 🫀 Consider LV function assessment in unstable angina, especially if symptoms, ECG changes or clinical findings suggest myocardial dysfunction.
- 🧪 If managed conservatively without angiography, consider ischaemia testing before discharge to quantify inducible ischaemia and guide further management.
- 📋 Ensure a clear written plan for antithrombotics, BP, lipids, diabetes, renal function, follow-up blood tests and cardiology review.
9️⃣ Secondary Prevention - long-term survival gains
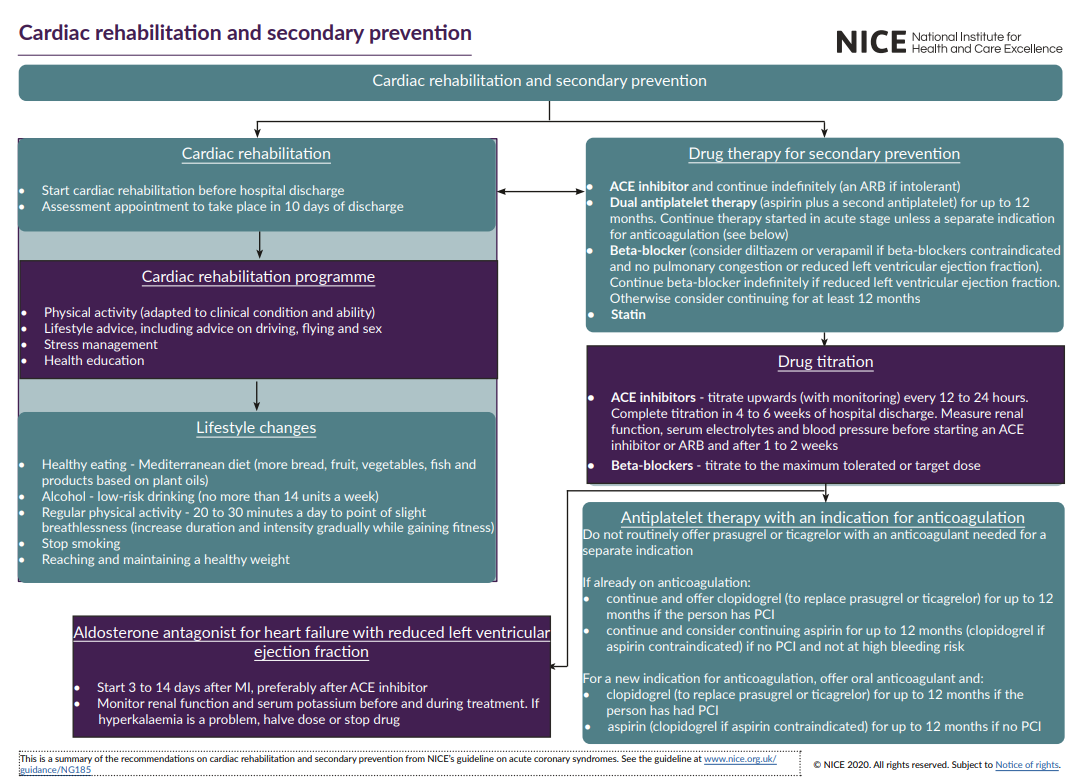
- 💊 DAPT: aspirin plus selected P2Y12 inhibitor is usually continued for up to 12 months; shorten if bleeding risk is high, or extend only if specialist-directed.
- 🧴 Statin: continue high-intensity statin long-term; consider add-on lipid-lowering therapy if not at target on specialist or local pathway.
- 💊 ACE inhibitor: start once haemodynamically stable after MI and continue indefinitely if tolerated; titrate to target or maximum tolerated dose.
- 🫀 Beta-blocker: offer after MI unless contraindicated; particularly important with LV dysfunction, arrhythmia or ongoing angina. Review duration and tolerability in follow-up.
- 🧪 MRA, e.g. eplerenone: consider if LVEF ≤40% with heart failure or diabetes; monitor potassium and renal function carefully.
- 🏥 Refer for cardiac rehabilitation and address lifestyle: smoking cessation 🚭, Mediterranean-style diet 🥗, graded exercise 🏃♂️, weight optimisation, BP control and medicines adherence.
|