
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Thyrotoxicosis and Hyperthyroidism
⚠️ Definitions
- Hyperthyroidism 🔥 = excess production and release of thyroid hormones (T3/T4) from the thyroid.
- Thyrotoxicosis ☢️ = clinical syndrome of thyroid hormone excess, from any source (thyroidal or extrathyroidal).
📊 Prevalence
- 🇪🇺 Europe: ~0.8% of population.
- 🇺🇸 USA: 1–3% prevalence.
- ♀️ More common in women (5–10x higher).
🔎 Causes of Hyperthyroidism / Thyrotoxicosis
- Graves’ disease 🌸 – Commonest cause (esp. women 30–50). – Diffuse goitre, ↑ RAI uptake, ophthalmopathy, pretibial myxoedema. – Autoantibodies: TSH receptor (TRAb). – Smoking 🚬 ↑ risk of eye disease.
- Toxic multinodular goitre 🪢 – Common in older adults, iodine-deficient areas. – Patchy uptake on RAI scan.
- Toxic adenoma (“hot nodule”) 🔥 – Solitary nodule, focal ↑ uptake on scan. – Causes classical thyrotoxicosis.
- Thyroiditis 🦠 – Often post-viral (subacute, painful). – Release of pre-formed hormone (NOT ↑ synthesis). – Features: tender thyroid, ↑ ESR/CRP, ↓ uptake on RAI. – Rx: NSAIDs/β-blockers; steroids if severe.
- TSH-secreting pituitary adenoma 🎯 – Rare. Raised TSH + T4. – Features: thyrotoxicosis + bitemporal hemianopia.
- Hashimoto’s “Hashitoxicosis” 🌀 – Transient thyrotoxic phase in autoimmune thyroiditis. – Antibodies: anti-TPO, anti-TG.
- Jod-Basedow effect 💊 – Thyrotoxicosis after excess iodine (contrast, amiodarone).
- hCG-mediated 🤰 – Hydatidiform mole, choriocarcinoma.
- McCune-Albright syndrome 🧬 – Triad: fibrous dysplasia of bone, café-au-lait spots, endocrine hyperfunction (incl. thyroid).
📊 Comparison Table – Common Causes of Thyrotoxicosis
| Feature | 🌸 Graves’ Disease | 🪢 Toxic Multinodular Goitre (TMNG) | 🔥 Thyroiditis |
|---|---|---|---|
| 👩 Typical Patient | Young–middle aged female (30–50), autoimmune background, smoker 🚬 | Older adults, long-standing goitre, iodine-deficient areas 🌍 | Any age; post-viral (subacute), postpartum, or drug-induced 💊 |
| 🩺 Clinical Features | Diffuse goitre, bruit, ophthalmopathy 👁️, pretibial myxoedema | Nodular, irregular goitre; no eye disease | Painful/tender thyroid (subacute) OR painless (silent, postpartum) |
| 🔬 TFTs | ↑ Free T4/T3, ↓ TSH | ↑ Free T4/T3, ↓ TSH | Early: ↑ T4/T3, ↓ TSH → Later: hypothyroid, then recovery |
| 🧪 Antibodies | +ve TRAb (TSH receptor antibodies) ✅ | Usually negative | Anti-TPO ± Anti-TG (autoimmune forms) |
| 📻 Radioiodine Uptake Scan | Diffuse, homogenous ↑ uptake | Patchy/multiple “hot spots” 🔥 | ↓ Uptake (due to hormone release, not overproduction) |
| 🩻 Imaging | Doppler: ↑ vascularity (“thyroid inferno”) 🔥 | Irregular nodules on USS | Low uptake; USS may show hypoechoic areas |
| 💊 First-Line Treatment | Carbimazole / PTU; ± RAI; surgery if needed | RAI often preferred; surgery for large goitre | Symptomatic only (β-blockers, NSAIDs/steroids if painful) |
| ⚠️ Key Exam Pearls | Only cause with eye disease 👁️; smokers at higher risk | Commonest cause in elderly; no eye signs | Tender thyroid + ↓ uptake = classic! 📉 |

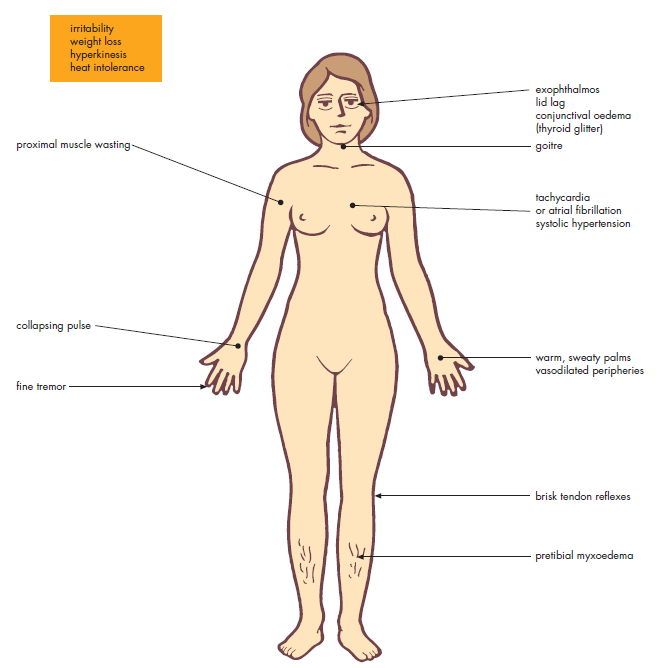
🩺 Clinical Features
- Weight loss ⚖️ despite ↑ appetite.
- Heat intolerance ☀️, sweating.
- Palpitations ❤️ (AF, tachycardia common).
- Neuro: anxiety, tremor, irritability.
- GI: diarrhoea, ↑ bowel frequency.
- Muscle: proximal myopathy 💪.
- Graves’ specific: Ophthalmopathy 👁️, pretibial myxoedema, thyroid acropachy.
🔬 Investigations
- ↑ Free T3/T4, ↓ TSH (except pituitary adenoma).
- TRAb positive → Graves.
- Other antibodies: anti-TPO, anti-TG (autoimmune thyroiditis).
- RAI uptake scan: diffuse (Graves) vs patchy (multinodular) vs focal (adenoma) vs ↓ uptake (thyroiditis).
- ECG: AF common → ↑ stroke risk 🧠.
- Other: mild ↑ Ca, ↑ ALP, ↓ K⁺ (periodic paralysis, esp. SE Asians).
💊 Management
- Symptomatic: – Propranolol 20–40 mg TDS (also ↓ T4→T3 conversion). – Useful for tremor, palpitations, anxiety.
- Antithyroid drugs 💊 – Carbimazole (1st line UK): start 20–40 mg OD → titrate to euthyroid (usual maintenance 5–15 mg). – Propylthiouracil (PTU): preferred in 1st trimester pregnancy; also blocks T4→T3 conversion. – Regimens: titration vs “block & replace” (carbimazole + thyroxine). – Duration: ~12–18 months, then trial withdrawal. ⚠️ Major adverse effect: agranulocytosis (0.5%) → fever/sore throat = urgent FBC + stop drug.
- Radioactive Iodine (I-131) ☢️ – Single dose effective in most. – Contraindicated in pregnancy & breastfeeding. – May worsen eye disease → avoid in active Graves’ orbitopathy (esp. smokers). – Hypothyroidism common post-treatment → lifelong thyroxine.
- Surgery 🔪 – Indications: large obstructive goitre, suspicious nodules, relapse after drugs/RAI, or pregnancy contraindicating RAI. – Risks: recurrent laryngeal nerve injury, hypocalcaemia (parathyroid removal).
🤰 Hyperthyroidism in Pregnancy
- Specialist endocrine + obstetric care required 👩⚕️.
- 1st trimester: PTU (less teratogenic).
- 2nd–3rd trimester: Carbimazole (preferred to avoid PTU hepatotoxicity).
- Surgery: 2nd trimester safest if needed.
- Uncontrolled thyrotoxicosis ↑ risk: miscarriage, pre-eclampsia, IUGR, stillbirth.
🚨 Thyroid Storm (Medical Emergency)
- Severe thyrotoxicosis with fever 🌡️, tachyarrhythmias ❤️, delirium 🧠, multi-organ failure.
- Precipitated by infection, surgery, trauma.
- Rx: – IV propranolol/esmolol (rate control). – PTU high dose (600–1000 mg load, then 200–300 mg q6h). – Lugol’s iodine after PTU (blocks release). – IV hydrocortisone (stress dose). – Supportive (fluids, cooling, ICU).
📚 References
- NICE CKS: Hyperthyroidism
- De Leo, Lee & Braverman. Hyperthyroidism. N Engl J Med 2016.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery